International Team to Nyandarua, Kenya. 16-20 Nov 2025
HERNIA INTERNATIONAL MISSION TO KARIUKI MEMORIAL COUNTY REFERRAL HOSPITAL, NYANDARUA COUNTY, KENYA.
NOVEMBER 16-20, 2025. STATUS: COMPLETED
Coordinator: Dr. Gachara Boniface (Kenya), coordinator Samuel Wainaina (Kenya), Medical
Superintended Beatrice Mugure (Kenya), Team leader Thorbjorn Sommer (Denmark).
The International Team: Steve Lindley, (UK), Heidi Miller (USA), Thorbjorn Sommer (Denmark), Soeren Pedersen (Denmark), Clara Scheffmann Gosvig (Denmark), Lene Scheffmann Gosvig (Denmark).
Total: 6 volunteers

TECHNICAL REPORT
DATES AND LOGISTICS DEPLOYED:
Campaign conducted November 16-20, 2025.
ADULT PATIENTS: Hernias (inguinal, umbilical, ventral, inguinoscrotal), lipomas, hydroceles.
PEDIATRIC PATIENTS: Hydroceles, umbilical hernias, inguinal hernia.
CONSULTATION AND SURGERY PERFORMED:
Patients seen in consultation: 104
Number of cases performed: 93
Complications: one week after termination of the camps no complications has been seen according to Dr. Jairus Ochieng.
For statistics please see Power Point from Dr. Gachara Boniface previously posted on this website.
CAMPAIGN SUMMARY
JM Kariuki Memorial County Referral Hospital
The Hospital is a major referral center for about 700.000 people living in Nyandarua County. It is located 3,5 hours’ drive north of Nairobi. The Hospital is under constant
development with new departments and development of various health projects. The hospital consists of different departments: Surgical department, emergency department,
Intensive care (4 beds), medical care, vaccinations center, facilities for child-mother care,
maternity, laboratory and testing etc, CT and Ultrasound scanning facilities.
Concerning the surgical department there were two operation theatres, with two tables each of which three was used for the current Hernia mission, while the other was used for caesarean sections. Other types of surgery (like ortopedics) were directed to other hospitals during the Hernia mission. As such it was possible to perform 3-4
operations simultaneously, which we found very efficient, making it possible to discuss difficult cases across the room.
The Kenyan side of the team had done a very efficient job and they were prepared for the mission. During the mission we also had a visit from a TV Team together with the Governor who took his time to visit the hospital accompanied with the bishop and CEO´s of the region and hospitals The recording from the visit went on live TV during the mission. This created further knowledge among the community about the possibility to get surgery for hernias.
The video can be viewed here: https://www.facebook.com/reel/1297884622024993. We had a lot of good experineces from the mission last year, which made it very easy to continue our cooperation in developing fast track surgery.
The operating theatres were well equipped with air conditioning, allowing for a comfortable work
environment. Power cuts were rare and did not affect our work.
The hospital was equipped with three diathermy machines, and we monitors for patient surveillance in the recovery room/ICU donated by Private Hospital Molholm in Denmark. The Team members brought each what was possible to collect of up-to-date equipment (gowns, sutures, scalpels, drapes, dressings, meshes, local analgesics etc.). We had a terrific cooperation with the local anesthesiologists George, Esau and Daniel and Kariuki
making it possible to do surgery under general or spinal anesthesia. Local anesthesia was used in selected cases.
The General Surgeon at the Hospital Jairos Ochieng is a very hard working and skilled general surgeon, and we had a very inspiring and joyful time together discussing treatment options in individual patients, indications for surgery and of course also technical aspects of Hernia surgery.
We did ward rounds every morning to see the postoperative patients from the previous days before discharging them. In between surgery we saw patients who requested screening for a variety of surgical/non -surgical diseases, and patients coming for check-up after surgery.
The patients were seen dressed in gowns ready for surgery in a room in front of the theatre where they were marked by the operating surgeon before the operation They were informed about surgery, written information about the surgery, operative procedure, risks etc. and consent of the operation was ensured. Cleaning between the shifts were swift, making it possible to do fast track surgery Patients were schedules to stay in the ward to the following day, where they were seen before
discharge.
THE TEAM
The team consisted of three surgeons: Steve Lindley (UK), Heidi Miller (USA) and Thorbjorn Sommer (Team leader Denmark). Anesthesiologist Søren Pedersen, (Denmark) Anesthetic Nurse Lene Scheffmann Gosvig (Denmark) and Clara Scheffmann Gosvig (assistant., Denmark) assisted with the procedures together with the local staff. Two months before departure we had 2 virtual Zoom meetings, with participation of our Kenyan colleagues, where we were introduced to each other, discussed the mission, the need of equipment to the Hospital.
TRAVEL/VISA/PERMITS
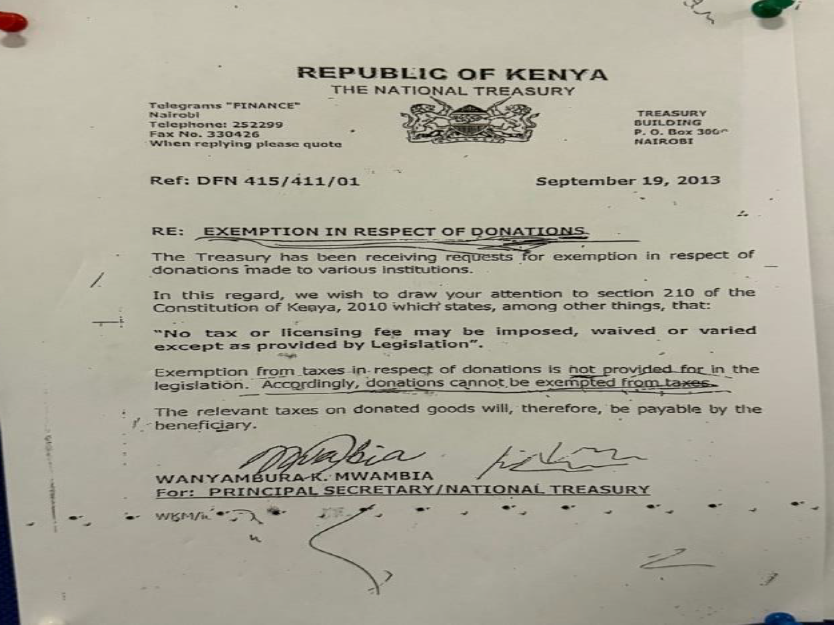
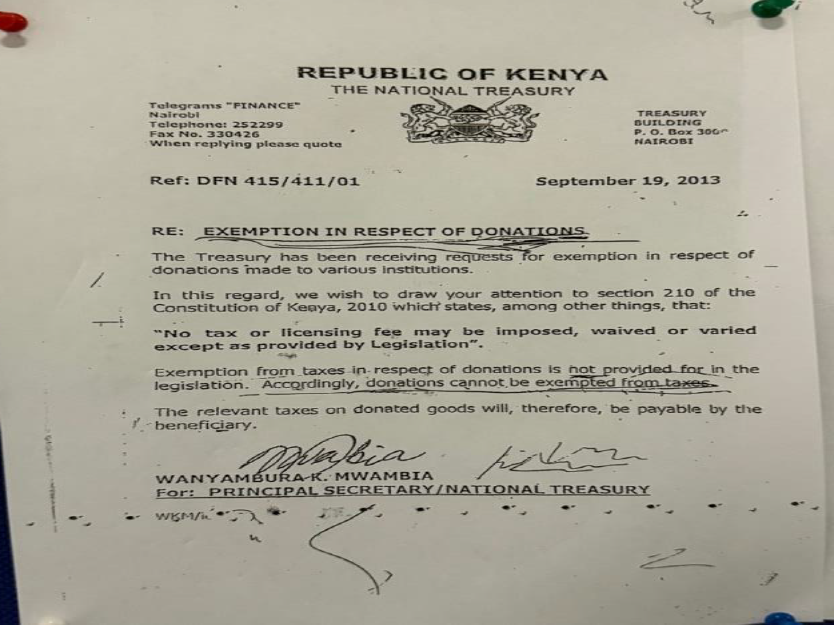
Travel to Kenya is easy since there are a lot of departures to Nairobi. eVISA must be obtained (online) before departure. Samuel did a terrific job securing Temporary Surgical License to the surgeons operating before arrival. We had a challenge to get out equiopment through customs, since there a new rules concerning donations in Kenya: Exemption for tax on donations should be acquired before arrival. Our Kenyan
staff had to pay a tax of 11.115 Shilling (86 USD) in Tax before we were allowed to take our
donated stuff with us to the Hospital.
SCHEDULE
Our routine included Breakfast at 7.30 AM before starting surgery at 8-8.30 AM. We had a lunch break at 2 PM, and finished the last surgery between 4 and 8 PM, depending on the
number of cases scheduled. Thursday night a party was arranged at the Hotel together with all the staff, local organization and everybody involved in the Hernia Camp with tasty food, a lot of good talks and the team members
were granted with gifts, which we all are very thankful for.
LOCAL STAFF
The local staff had done a significant job in recruiting patients using various channels such as posters, newspapers and radio advertising, ensuring we had a sufficient amount of patients. Especially after the news about Hernia surgery upon the governers visit secured a lot of patients, some coming from afar (+500 km away).
Arriving at the Hospital all patients were carefully registered and prepared before being seen by a surgeon prior to surgery, with evaluation and marking of the hernia. It was an important and primary focus of all staff to ensure patient safety from the first step.
Doctor Aisha and nurse Lucy were phenomenal to arrange everything logistically, kept the files in place, knew were the next patient was and where the previous should go.
The Medical Superintended Beatrice Mugure did a terrific job with competent overview of the organization. Extra personnel had been called in, so we were well equipped with competent staff from anesthesia, surgical and ward
assistance, making it possible to upscale the number of procedures. Safe check in was performed before initiating surgery. Working together with the local staff was a very positive experience for all of us, sharing expertise, skills, technical tips and ways to go forward in the care of
hernia patients as well as keeping a good spirit, lots of laughs, hugs and good humour.
EQUIPMENT
The Hospital was well equipped, and the Team brought what was possible for each member to collect from their home Hospitals of new equipment. Private Hospital Moelholm donated monitors for further use in the recovery/ICU rooms.
ANESTHESIA
The Theatres were equipped with ventilators and at each operative table, there was monitor with a pulse oximeter and a blood pressure cuff, and ECG. Anesthesia was obtained using Ketamine, Halothane, Propofol and Desflurane, spinal or local anesthesia. The majority of patients received local blockage with Marcaine as post operative pain treatment together with Paracetamol and Ibuprofene. Having an anethetic team with us working together with the local anesthetisist was very valuable, and different ways to do anestesia in safe ways were discussed and developed.
ASEPSIS AND SURGICAL MATERIAL
All patients had washed before arrival for surgery. At the hospital they were washed with
appropriate antiseptics, hair was removed, the site of operation was preoperatively marked on the skin and local anesthesia was applied. All patients received a single dose of Ceftriaxone as SSI profylaxis. The local staff practiced aseptic procedures making it easy to secure clean procedures. Sufficient surgical material boxes were available.
ACCESSIBILITY FOR THE POPULATION
Before our arrival, the Hospital had conducted an information campaign with information about the possibility of hernia surgery. The patients paid a small fee, what they could afford, some came a
long way to be operated (many hours of transportation).
ACCOMODATION IN NUANDARUA
Again we stayed at the nice 818 Hotel situated 1 km from the Hospital, making a short morning walk possible. The Hotel had a very nice staff, nice spacious rooms with aircon, clean bathrooms, a nice restaurant with a variety of local and international meals. However, the best was a Tusker Beer after long working hours.
CONCLUSION
Strengths:
The Hospital is not too far away from Nairobi Airport, reducing time for transportation to a
minimum. Transportation is swift and well organized. Patients came from far away, and the standard at the facility made it easy to do high-volume Surgery with good quality in every aspect. Accommodation is nearby so no time is wasted on transportation.
The staff is very well educated and a tremendous help in assisting us with everything. They have the capacity to raise awareness of Hernia surgery, planning a comprehensive surgical camp and secure patient safety in a high-volume setting. It is highly recommended to further develop Hernia Camps in Nyandarua, since all capacities for further hernia surgery is present. There is also a wish to do laparoscopic hernia surgery in the future, and if it would be possible to provide laparoscopic equipment it would definitely be the place to do it.
Things we might do differently:
Among a variety of strategies we worked on: preparation for each case in the theatre making sure all equipment was available, which kind of anesthesia was intended and what kind of hernia was to be repaired in which patient – should be known before bringing the patient to the theatre.
- Keeping things in order on the tables, ensuring a low risk of substitution of drugs and
instruments. - having a pecific contact person in the morning when doing the reounds to identify patients from the previous day, ensuring everybody was seen would be a good value as well, shortening time to the rounds making more time at the theatre possible.
- engagement of local media, especially TV shortly before the mission would be of great value concerning patient recruitment. Videos taken this year could be used on social media referring to the possibility of surgery in Nyandarua.
In conclusion we again highly recommend Hernia Missions conducted on an annual basis in Nyandarua from Hernia International.
On behalf of the Team 2025
Yours sincerely,
Thorbjorn Sommer
Head of International Team to Nyandarua
November 2025