American Team to Herona Hospital, Uganda. March 2026
American Team to Mikono District, Uganda.
March 2026
REPORT
Dates: March 23 through March 27, 2026 Host: Herona Community Hospital
Team members: Alan Kravitz, MD, Chandra Hassan, MD

Lichtenstein Hernia Surgical Mission at Herona Community Hospital
Herona Community Hospital is located in Kisoga, Mukono District, about 40 km east of Kampala, the capital of Uganda. The hospital serves a wide rural catchment area where most residents live in poverty and have limited access to surgical services. Many patients suffer from treatable conditions such as hernias but are unable to afford surgery due to financial constraints and long travel distances to referral hospitals.
In rural hospitals such as Herona, much of the care is rendered by non-specialist physicians. These general doctors provide a wide array of medical and surgical care including primary care, pediatrics, obstetrics, C-sections, and basic trauma care.
Our goal with this mission was to attempt to teach these doctors basic hernia repair techniques so that they could leverage these new skills from our visit to perform surgeries on their own.
Dr. Henry Garvin, the hospital director, arranged for several local physicians to assist and perform hernia surgeries under the instruction of Drs. Hassan and Kravitz.
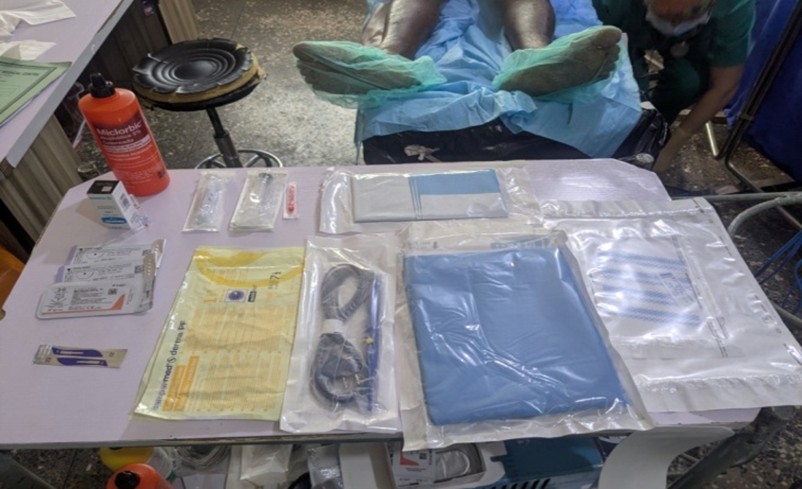
The operating rooms were well supplied with sutures, and the hernia meshes had been prepared and supplied by nurses at the hospital, from low-cost material provided by AMSA Plastics.
We were impressed with the basic surgical skills of the local doctors. We felt they were equivalent to most PGY-3 residents in the USA. They were very enthusiastic about learning the Lichtenstein technique as well as basic umbilical hernia repairs.
They assisted, and then were given primary surgeon roles as the week progressed. There were even a few cases where they assisted each other without supervision.
A total of 42 patients were treated. These patients had mostly inguinal and femoral hernias, as well as some umbilical and epigastric hernias. Most of these cases were done under spinal anesthesia.
Since we have left, they have done a few cases on their own. We have sent them instructional videos and have remained in touch. They are keeping a log of their cases, and hopefully we will be able to use this model in other locations to expand the impact that Hernia International can make on the communities that we serve.


Slovenian-Austrian-Swiss-Team Mission
St. Gaspar Hospital, Itigi, April 19th-25th
TANZANIA 2 0 2 6

Hernia International Foundation
Following political unrest in Tanzania in November 2025, we had to postpone our planned mission for that year, and we were pleased it could take place in April 2026.
Itigi is a town in central Tanzania, located within Itigi District in the Singida Region. It comprises the wards of Itigi and Itigi Majengo, which had a combined population of 21,777 according to the 2012 national census. The town is crossed by the unpaved trunk roads T18 (linking Manyoni to Tabora) and T22 (connecting Singida Region to Mbeya Region). We reached Itigi by minibus from Dodoma, following a domestic flight from Dar es Salaam to Dodoma. Itigi is also a stop on the Central Line of Tanzanian Railways, though rail travel is notably slow.
St. Gaspar Hospital was established, and continues to be managed and supported, by the Congregation of the Missionaries of the Precious Blood, an organization with roots in Italy. Recognizing the significant need for accessible healthcare in the area, the hospital was inaugurated in 1989. Today, it serves as a key regional referral center, guided by its mission to “cure, educate, and console.”
The hospital employs 28 doctors, 103 nurses, and over 100 additional staff members. As a Level 5 facility (on a six-level scale), it is exceptionally well equipped, with clean, modern buildings that include endoscopy services, blood transfusion capabilities, a CT scanner, an ICU and IMC, a farmacy that produces its own cristaloid solutions for i.v. infusions and four operating theaters (two major and two minor). None of us had previously worked in such a well-equipped hospital during a Hernia International mission.
Our team consisted of ten members: three surgeons, two anesthesiologists, one radiologist, one scrub nurse, one nurse anesthetist, one ENT specialist (who is also a maxillofacial resident), and one dental student. Local consultant
surgeon Dr. Seif Nuru, together with his team of surgical residents, actively contributed to both the clinical work and the educational activities.
We brought 240 kg of equipment and medications in 11 bags and were pleased that the import process went smoothly without complications at customs. However, for the first time—despite the charitable nature of our work—each doctor was required to pay a USD 200 fee for a working permit issued by the Medical Council of Tanganyika.
The daily schedule at St. Gaspar Hospital was well structured and supportive. Each day began with a morning prayer at 7:30 a.m. for all hospital staff, followed by a scientific lecture for doctors. Our team delivered four lectures covering hernias, bowel cancer, proctology, and anesthesia. After breakfast, surgeries typically began at 9:30 a.m. (earlier on Fridays), with two operating tables running simultaneously and only brief interruptions for emergencies.
The workday usually ended around 5:00–6:00 p.m., followed by team briefings during dinner at 7:30 p.m.


In addition to treating five patients with goiters (all managed with one-sided total lobectomy, including two big recurrent goiters, using Ligasure and optical magnification for nerve identification), we operated on 18 hernia patients—eight infants and ten adults, including inguinal, large scrotal, and complex incisional hernias. The youngest patient was two years old. Lichtenstein repair was used in the vast majority of adult patients with inguinal hernia, employing LDPE meshes.


After thorough evaluation, including gastroscopy and CT imaging, we made the considered decision to perform a gastric resection on a patient with a bleeding GIST tumor of the stomach fundus. Although such a procedure is unusual for this type of mission, it was deemed life-saving for a relatively young patient and therefore justified.
We also carried out several emergency procedures, including surgery for peritonitis caused by a perforated appendix and, in collaboration with local doctors, the treatment of a sharp abdominal wall injury in an infant. Supporting and involving local surgeons in procedures was an important goal this year, and we hope to expand this collaboration further in future Itigi missions.
Operating on two tables allowed us to complete 26 procedures over four days.
Scrub nurse Jihan provided excellent support, continuing concern for sterility in Ots – the strong work carried out by her colleague Manuela Logan on previous missions. Our ENT specialist, maxillofacial resident, and dental student were highly engaged in the dental clinic, where six demanding tooth extractions, treatment of injuries and other examinations and procedures were successfully performed.

Maria carried out numerous ultrasound examinations using her portable device, which proved highly valuable preoperatively in cases of goitre and other conditions (such as hernias and hydroceles), as well as occasionally postoperatively. She was also engaged in interpreting CT scans for other patients, including those with stroke and intracranial injuries.

We were grateful to complete the program without any major complications, which we attribute to a well-managed schedule that avoided overcrowding. The minor complication, we had was a SSI in an obese (BMI>35) adult female after appendix perforation and 4-quadrant peritonitis. In the following outpatient treatment she received local skin wound management and prolonged oral antibiotics. Sufficient time was dedicated to each procedure, ensuring careful, unhurried care, particularly for HIV-positive patients (approximately 4–5% in this region of Tanzania).
Special thanks go to the outstanding anaesthesia team—these procedures would not have been possible without their support. In OT1, spinal anaesthesia was most commonly used, with general anaesthesia administered in some cases, whereas procedures in OT2 were performed exclusively under general anaesthesia. They helped out in many others surgeries, performed by local surgeons, when needed.

We were comfortably accommodated in the so called St. Gaspar Motel within the hospital complex and had there both breakfast and dinner (sometimes also lunch).
The positive working environment and strong sense of camaraderie were the result of thorough mission preparation over several months, with special thanks to Dr. Seif Nuru, Father Justin, medical director Dr. Simon, vice medical director Dr. Hilda and all those involved.
Team Members:
Prof. Mirko Omejc, MD, PhD – consultant surgeon, Ljubljana Medical Centre, Slovenia.
Prim. Miran Rems, MD, MSc – consultant surgeon, Slovenia.
Katalin Wiese, MD – consultant in anaesthesia, critical care and emergency medicine, Landeskrankenhaus Feldkirch, Austria.
Hannes Lienhart, MD, MSc DM – consultant in anaesthesia, critical care and emergency medicine, Landeskrankenhaus Feldkirch, Austria.
Marija Jekovec, MD – consultant radiologist, Ljubljana Medical Centre, Slovenia.
Anže Jerman, MD – ENT consultant and maxillofacial resident, Ljubljana Medical Centre, Slovenia.
Avelina Temba, MD, consultant general surgeon, Korogwe, Tanzania. Daniel Ketterer, anaesthesia nurse, Landeskrankenhaus Feldkirch, Austria.
Jihan Göggel, scrub nurse, Krankenhaus Grabs, Switzerland.
Nika Blažka Gorjanc – dental student, Medical faculty, Ljubljana, Slovenia. Asist. prof. Jurij Gorjanc, MD, PhD, FRCS, FEBS AWS – consultant surgeon, team leader, Klinikum Klagenfurt, Austria.

Our sponsors:
Bernhard und Karin Chwatal Medical Center Gorjanc
Implantološki institut / Implant Institute Chemomedica Wien
LKH Feldkirch Spital Grabs Kirurgija Bitenc Stiftspfarre Gurk,
Kan. Msgr. Mag. Gerhard Kalidz, Gurk
Mag. Dr. Walter Ganster – Steuerberater Völkermarkt Goldhaubenfrauen Gurk
Gurker Bänderhutfrauen Friesacher Bürgerfrauen
Spanish Team to Freetown, Sierra Leone. February 2026

POLICE HOSPITAL FREETOWN MISSION 2026
TECHNICAL REPORT
DATES AND DEPLOYED LOGISTICS
- Mission Dates: January 31 to February 11, 2026.
- Adult Patients: Inguinal, umbilical, and ventral hernias; goiters, lipomas, and sebaceous cysts.
- Total Procedures: 171.
- Total Patients: 158.
- Complications (7 days post-op): 1 scrotal hematoma, 1 acute urinary retention (AUR), and 1 metamizole allergy.
- Complications (1 month post-op): 2 reported complications: 2 seromas

CAMPAIGN REPORT
1. MISSION MEMORANDUM
A. THE SETTING
Sierra Leone faces one of the most complex healthcare scenarios in West Africa, characterized by a high burden of communicable diseases, extremely unfavorable maternal and child health indicators, a fragile healthcare system, and growing challenges derived from non-communicable diseases. Despite recent progress in access to essential services, health outcomes remain suboptimal, and significant territorial and socioeconomic inequalities persist.
Communicable diseases constitute the primary cause of death and illness in the country. Malaria is the single largest healthcare concern, accounting for approximately 38% of all hospital admissions. Tuberculosis remains a major public health issue, with an estimated three new infections per 1,000 inhabitants annually. The national HIV prevalence stands at around 1.5%, remaining relatively low compared to other countries in the region, although significant challenges persist regarding early diagnosis and access to treatment.

The country was severely affected by the most extensive Ebola virus disease epidemic in recent history. Between May 2014 and March 2016, 8,706 infected individuals were recorded, of whom 3,590 died. This episode not only caused high direct mortality but further weakened an already vulnerable healthcare system, affecting public trust, the availability of professionals, and the continuity of essential services. The risk of epidemics and other public health events remains high, given structural limitations in epidemiological surveillance and response capacity.
In the field of maternal and child health, Sierra Leone presents some of the most concerning indicators worldwide. It is estimated that the country has the highest maternal mortality rate globally. Infant mortality is also very high. In 2014, nearly one-third of children under the age of five showed signs of stunting, a reflection of chronic malnutrition. Anemia constitutes a severe public health problem, affecting approximately 70% of pregnant women and 76.3% of children under five. These data evidence significant deficiencies in nutrition, prenatal access, safe obstetric care, and basic pediatric services.
Simultaneously, non-communicable diseases and injuries are emerging as a growing health concern. This phenomenon is linked to the high prevalence of behavioral risk factors such as tobacco use, unhealthy diets, sedentary lifestyles, and harmful alcohol consumption. Pathologies such as cardiovascular diseases, cancer, diabetes, and chronic respiratory diseases, as well as trauma and mental health disorders, increasingly contribute to premature mortality and disability. This situation creates a “double burden of disease,” where communicable and non-communicable pathologies coexist within a healthcare system with limited resources.
While progress has been made in expanding access to essential health services, health outcomes remain insufficient nationwide. Significant inequalities persist in access and health results across different districts and income levels. Geographical, economic, and structural barriers hinder equity in healthcare delivery.
In response to these challenges, the country has developed national strategies and plans aimed at increasing access and improving the quality of essential services, with the objective of saving lives, preventing disease, promoting health, and providing curative care and psychosocial support to those affected. However, consolidating these efforts requires sustained investment, institutional strengthening, the development of healthcare human resources, and improved system governance.
Overall, Sierra Leone faces a complex healthcare landscape defined by high epidemiological vulnerability, structural weakness of the health system, and profound social inequities. International cooperation and local capacity building remain fundamental elements for advancing toward a more resilient, equitable, and sustainable healthcare system.

The Police Hospital, located in Kingtom, Freetown, is a healthcare center belonging to the Sierra Leone Police (SLP) that has historically provided medical care primarily to police members and their families. Its primary function is to ensure the physical and mental well-being of police officers, providing preventive, curative, and emergency services, as well as occupational health support, vaccination, and medical response during security operations. Additionally, the hospital is part of the Police Medical Services Directorate, which collaborates with national and international health institutions to expand its reach and strengthen its care capacities.
In recent years, the Police Hospital has undergone a process of transformation and service expansion, evolving from a limited center for police personnel to a hospital with broader care capacity and community impact. This evolution has been driven by both the SLP leadership and partnerships with international medical organizations. One of the most notable initiatives was the collaboration with the Surgeons in Action Foundation, thanks to the efforts of Dr. John Konteh, which has carried out multiple free surgical campaigns at the center, providing specialized care not only to police officers and their families but also to the vulnerable civilian population. These campaigns have enabled hundreds of surgical procedures—including general surgery—and provided key medical equipment, such as anesthesia machines, tangibly improving the hospital’s technical capacity.

Beyond these campaigns, the center has expanded its infrastructure with the opening of services such as an ophthalmology clinic and the construction of a morgue, as well as the stated intention to develop a nursing school to train local healthcare professionals. These improvements reflect an institutional leadership committed to strengthening the hospital’s resolving capacity and consolidating it as a relevant healthcare resource within Freetown. Another important aspect is the use of the Police Hospital as a space for clinical training and teaching. Under the direction of the Medical Superintendent, the hospital has served as a learning platform for local healthcare professionals, contributing to reducing dependence on foreign personnel and gradually raising the medical competencies available in Sierra Leone. Although the Police Hospital is not a direct part of the network of public hospitals managed by the Ministry of Health and Sanitation (such as Connaught Hospital or Princess Christian Maternity Hospital), its role has expanded through public-private partnerships and international cooperation, especially in contexts where the need for specialized services exceeds the capacity of traditional public hospitals.
Our activity was developed exclusively in the surgical block, located in a two-story building separate from the rest of the complex. This building features 3 consultation areas (one of them being Dr. Konteh’s office) and 3 hospitalization wards; we used the two larger wards for men and the smaller one for women, typically for thyroid pathologies. The total capacity is 28 beds, which were used entirely for the campaign, occupying the whole floor for our work. At the end of the hallway is the access to the operating room area, which maintains a sterile circuit with two large ORs connected by a shared sterile room and hand-washing station. Likewise, in the hallway, there is a room with a long table used for our meals and coffee, in direct contact with OR 1.

There is a new anesthesia machine, a Dräger Atlan A300 model, featuring mechanical ventilation (VC and PC), a sevoflurane vaporizer, and perfectly functioning capnography. The operating rooms are equipped with split air conditioning units, allowing for comfortable work over many hours despite high outdoor temperatures. However, power outages occur frequently, requiring the units to be restarted and causing moments of sweltering heat. The sterile area is where local staff work diligently to sterilize gowns, drapes, and instrument sets. On the upper floor, there is a nursing duty room used as a storage area for surplus material from previous campaigns and as a changing room for the volunteers.
As per our campaign custom, and despite initial reluctance from local staff, we structured OR 1 (the larger of the two on the left) to accommodate 3 surgical tables. This setup, while not excessively spacious, was functional and allowed enough room for patients to enter on stretchers (Photo 1) so we could work together. Based on the experience gained from our previous 8 campaigns, staying together, working together, and taking breaks for meals and coffee as a group is fundamental to the work environment and team relationship. OR 2 was utilized as a Kanban area.
B. THE TEAM (Group Members)
The team specifically comprised General Surgery specialists Eduardo Perea, Manuel Bustos Jiménez, Abdul Razzak Muchref Al Dandal, Carlos Javier García Sánchez, Jose María Álamo Martinez, and Ángela de Jesús Gil; Surgical Resident Beatriz de los Ángeles Ruiz García; Anesthesiologists Alejandra Abasolo Ibañez, Ordoño Rodrigo Alonso Tuñon, and María del Mar Martínez Gómez; and Daniel Luis Nadales Muñoz as the Nursing lead. This year, an additional surgeon joined the team to manage outpatient consultations and morning ward rounds without delaying operating room (OR) activity, as well as to relieve the more experienced surgeons during afternoon shifts without affecting the surgical schedule.

Despite initial reservations regarding such a large group, it was proven that in a facility with such extensive local support and availability, a large team capable of operating on three tables simultaneously—while simultaneously triaging patients, managing discharges, and addressing unforeseen events such as emergencies or gastrointestinal illnesses among team members—resulted in a success in both the volume and the quality of care provided.
C. LOCAL STAFF
The hospital provided a large and available local team; the experience was overwhelmingly positive in terms of the involvement of both OR and ward staff, exceeding that of previous campaigns. Participants included:
- Dr. John Konteh: His role was exceptional, managing massive patient recruitment with precise pathologies, providing follow-up for post-operative patients, resolving emergencies, and assisting the volunteer physicians with basic needs, accommodation, transport, and currency exchange. His 24/7 availability and the provision of missing materials ensured a continuous sense of institutional backing from the Police and the center.
- Security Personnel: They provided transport from the hotel and accompanied the team during consultations and within the hospital. Special mention goes to Abu Marah, who was always helpful and managed traffic control.
- Police Nurse Liaison: Mohamed served as the campaign coordinator and our primary point of contact, maintaining direct communication with Dr. Konteh. Although initially shy, his efforts were essential for the seamless operation of the mission.
- Outpatient Assistant: Marie provided an admirable spirit and joy to the center. She prepared the consultation rooms, ensured a constant supply of fresh water, and managed the arrival of new patients for screening.
- Ward Staff: 4 to 6 nursing assistants/nurses monitored patients postoperatively and managed intravenous access. Nurses Davide and Vintu were particularly notable for their dedication to patient mobilization, monitoring vital signs, and pain control, as well as assisting in consultations.
- Operating Room Staff: 2 to 7 members performed various roles, from cleaning to porterage, ensuring the agile transfer of patients. Two nurses possessed basic anesthesia knowledge (Yabah and Francis), and two others served as circulating or scrub nurses. Their constant presence throughout the day was a vital asset.
- Sterilization Lead: Kabba was responsible for the sterile supply, constantly providing gowns, drapes, and instruments for three surgical tables, even as our own supplies began to dwindle.
D. EQUIPMENT
The OR consists of three surgical tables. There is one electrosurgical unit (ESU) that only supports a single terminal. Various sutures remained from previous campaigns. No surgical meshes are available locally. Two monitors with pulse oximetry and BP cuffs are provided.
E. ANESTHESIA
The OR is equipped with a Dräger Atlan A300 ventilator capable of VC and PC mechanical ventilation, a Sevoflurane vaporizer, and perfectly functioning capnography. Oxygen cylinders (up to 4 or 5 available), saline solution, and IV catheters are on-site. The supply cabinet contains some ampoules of norepinephrine, bupivacaine with dextrose, and epinephrine. Two monitors are available, though their operation is inconsistent.
F. ASEPSIS AND SURGICAL MATERIAL
Basic surgical sets contain sufficient but deteriorated instruments. Organization was challenging as we had to include all the instrument sets we intended to use. However, sterilization was completed within an hour, allowing for rapid turnover. Cloth gowns and drapes are similarly autoclaved. Given the high volume of interventions, it is recommended to bring additional gowns and drapes, as sterilization times sometimes lagged behind demand. Bringing a portable ESU is advisable; in this mission, we brought an ESU and a Ligasure device to enable simultaneous surgery on three tables.

G. ACCESSIBILITY FOR THE POPULATION
The hospital is highly affordable and accessible; patients were not charged for surgery or admission. Imaging and laboratory tests are available at a separate facility for a reasonable fee. The team noted that the treated population was in significant need and lacked easy access to alternative healthcare. All medication was provided by our team, with surplus stock donated to Dr. Konteh.
H. LIFE IN FREETOWN
The preparation and success of the campaign at Police Hospital were inextricably linked to the collaboration of Dr. Konteh and Mohamed. They actively participated in logistics, including airport pickup and negotiating rates at local hotels. We noted that the country and the campaign in general were more expensive than in previous years. The Jam Hotel was selected for its proximity and price.
- Day 1: Departure from Seville to Malaga by bus, followed by a flight. Arrival in Freetown at dawn after a 5-hour layover in Casablanca. Dr. Konteh facilitated customs and security, avoiding fees. After taking the ferry to the capital, the team went directly to the hospital at 8:30 AM to set up the OR and screen patients. Over 200 patients were waiting. While Anesthesia and Nursing organized 22 suitcases of equipment, the surgeons divided into teams to perform screenings and complete surgical schedules. The day ended at 6:00 PM.
- Day 2: Reception at the Police Headquarters followed by a 10-minute drive to the hospital. Due to roadworks and chaotic traffic, walking is discouraged. Consultations and surgeries began on three tables. The first day concluded with 24 patients treated.
- Days 3–10: Incessant OR activity due to a “call effect” that drew a high volume of patients. Over 250 patients were seen in consultation. Local staff showed impeccable commitment. On Saturday the 7th, the team visited the MercyShip Africa, establishing a cordial relationship to ensure follow-up for patients remaining on the waiting list.
- Day 10: On the way to the center, the team assisted a 14-year-old girl struck by a motorcycle. The final 12 scheduled cases were completed in the morning. At the last moment, a painful incarcerated umbilical hernia arrived as an emergency and was treated. Following a brief visit to a local market and a farewell dinner with the hospital staff, the team departed for the airport at night.
I. IMPLEMENTATION OF IMPROVEMENTS
As in the previous year, we have included this section, which we consider essential as it is the result of 9 campaigns conducted by this family of volunteers alongside Surgeons in Action.
The role of our local counterpart, Dr. Konteh, has been absolutely vital for the development of the campaign and the achievement of results. His involvement allowed for pre-arrival coordination and the transportation of patients from remote locations (up to 300 km away) for surgery. Similarly, we have secured the assistance of Mohamed, who will manage a local terminal to provide support and follow-up for patients who underwent thyroidectomies.
Based on our satisfaction surveys from the previous year, we have improved patient care, the protection and defense of privacy, and communication and information delivery during consultations. We also identified affordable pharmacies where patients can obtain Thyroxine. Simultaneously, two scientific projects were conducted by medical students from the University of Seville, focusing on the role and impact of cooperation campaigns on local healthcare activity.
We continue to refine our patient CHECKLIST system, which we will share with other Surgeons in Action missions. This tool facilitates patient screening and ensures compliance with quality standards.
A color-coded identification system using wristbands and stickers has been implemented. This system highlights potential surgical or anesthetic difficulties and provides visual alerts for HIV-positive patients or those with specific allergies.
J. PATIENT FOLLOW-UP
The Surgeons in Action 2026 project is designed, as it was in previous years, to ensure the follow-up of all surgical patients. Thanks to the collaboration of Dr. Konteh and Mohamed, a monitoring plan has been established, including follow-up calls for thyroid patients to monitor clinical symptoms and treatment adherence.
Additionally, a WhatsApp group has been created for hernia patients to address concerns and ensure proper follow-up. Wound reviews will be conducted at the local hospital by trained nursing staff, and thyroid treatment follow-up will be managed by the hospital’s Endocrinologist for the patients operated on during this mission.
K. RESULTS
| Variable | Resultado (N = 158) |
| Sexo masculino | 127 (80.65%) |
| Edad (Media [SD]) | 44.22 [±19.16] años |
| Color (Triage) | Verde: 5 (3.2%) Amarillo: 48 (31.0%) Azul: 84 (52.3%) Rojo: 21 (13.5%) |
| Alergias | 2 (1.29%) |
| HTA | 20 (12.90%) |
| Diabetes (DM) | 5 (3.23%) |
| Medicación domiciliaria | 25 (16.13%) |
| Diagnóstico | N (%) |
| Hernia inguinal | 98 (63.23%) |
| Hernia inguinal bilateral | 13 (8.39%) |
| Hernia ventral | 10 (6.45%) |
| Lipomas y tumores blandos | 1 (0.65%) |
| Bocio | 21 (13.55%) |
| Hidrocele | 5 (3.23%) |
| Criptorquidia | 1 (0.65%) |
| Hemorroide | 1 (0.65%) |
| Frenillo | 1 (0.65%) |
| Quiste sebáceo | 1 (0.65%) |
| Onfalocele | 1 (0.65%) |
| Procedimiento | N |
| Liechtenstein | 103 |
| Nyhus | 0 |
| Rives | 5 |
| Hemitiroidectomía | 10 |
| Tiroidectomía subtotal | 3 |
| Tiroidectomía total | 7 |
| Hidrocele (cirugía) | 5 |
| Orquiectomía | 1 |
| Exéresis | 4 |
| Herniplastia preperitoneal | 1 |
| Drenaje de absceso | 0 |
| Herniorrafia | 5 |
| Hemorroidectomía | 1 |
| Istmectomía tiroidea | 1 |
| Variable | N (%) |
| Incidencias intraoperatorias | 3 (1.94%) |
| Reintervenciones | 0 (0%) |
| Náuseas | 4 (2.58%) |
| Retención urinaria | 2 (1.29%) |
| Sangrado herida | 0 (0%) |
| Hematoma | 1 (0.65%) |
| Seroma | 0 (0%) |
| Parálisis recurrencial (disfonía) | 1 (4.76%)* |
| Tiempo | N (%) |
| Ambulatoria (0 días) | 131 (84.52%) |
| 1 día | 23 (14.84%) |
| 2 días | 1 (0.65%) |
| 3 días | 0 (0%) |
L. SCIENTIFIC ACTIVITY
Data has been collected for two Undergraduate Dissertations (Final Degree Projects) by two final-year medical students from the University of Seville. The purpose of these studies is to analyze the impact of cooperation campaigns on the host centers and populations, evaluating the evolution of healthcare delivery models and the potential application of Artificial Intelligence (AI) in surgical cooperation missions.
The analyzed data and resulting conclusions will be shared with both Surgeons in Action and the leadership of the host center.

2. CONCLUSION
Strengths of this location:
- Strategic Location: High density of population in need with limited access to surgical personnel.
- Exceptional Local Collaboration: The local hospital staff is accustomed to several campaigns per year, making them highly familiar with this type of medical activity.
- Institutional Network: A significant number of Spanish foundations and NGOs operate in Freetown, which aids in reaching vulnerable populations. This allows for high patient recruitment and a reliable local counterpart that facilitates patient preparation and follow-up.
Objectives for Improvement:
- High Campaign Costs: Expenses related to transportation, lodging, and meals remain high.
- Endocrine Surgery Specialization: It is recommended to include an endocrine surgeon. Although hernias are the primary objective, the area is endemic for goiters and Graves’ disease. While the local staff maintains the hernia OR, they are particularly interested in resolving thyroid issues, which are rarely addressed in the capital.
- Energy Sources: Ensure the availability of additional energy sources (electrosurgical unit or Ligasure for goiters).
- Team Capacity: The hospital accommodates large, multidisciplinary teams effectively.

3. BUDGET (Breakdown of Expenses)
COST PER PARTICIPANT:
- Round-trip flights (including medical equipment check-in): €1,100
- Bus transport: €50
- Ferry: €100
- Accommodation (Hotels): €400
- Meals: €200
- Local transport and others: €0 (Funded by Police Hospital)
Total cost per participant: €1,850
TOTAL CAMPAIGN COST: Approximately €20,350
Fdo: Eduardo Perea del Pozo Responsable de la campaña Police Hospital 2026
Cirujanos en Acción
Spanish Team to Makurdi, Nigeria. Nov 2025
MAKURDI CAMPAIGN, NIGERIA. NOVEMBER 2025
- INTRODUCTION
On this occasion we organized in collaboration with Hernia International a campaign at the Bishop Murray Medical Center in Makurdi, Nigeria, where at least three previous campaigns have already been carried out, the most recent one in May 2025.
The core group initially consisted of four members from a campaign carried out the previous year in Sierra Leone. Thanks to a call made by Dr. Butrón Vila to volunteers from the Cirujanos en Acción Foundation, the group was quickly completed, ultimately forming a team of 14 people.
- TECHNICAL REPORT
2.1 DATES AND LOGISTICS
The campaign was organized for the week of November 14 to 23, 2025.
We assembled a team of 14 people with the idea of working on three operating tables, based on the information provided by members of the previous campaign: one table for general surgery (hernias) with spinal anesthesia, one table for thyroid surgery with general anesthesia, and another table for pediatric surgery with general anesthesia.
We purchased the airline tickets through Ángelis, an agent from Halcón Viajes who usually manages this process for the Foundation’s campaigns. Six people departed from Madrid, five from Barcelona, and two from Vienna. We all met in London and from there took the flight to Abuja. Once in Abuja, we met Salifuo, a team member who traveled independently from Niger. Following the advice of the previous team, we hired a bus service from Abuja to Makurdi for €85 per person (round trip) through Austin Ella, our local contact in Nigeria for the campaign.
As with the previous campaign, the main problem was obtaining visas. Although on this occasion the electronic visa was available at a cost of €256 for a tourist visa, the Nigerian Immigration Service operates erratically. We encountered three scenarios: some obtained the visa without major difficulty in less than 24 hours; others were initially denied and had to reapply (and pay again) to obtain it; and a third group received no response at all (neither approval nor denial). Despite having initiated the process in September (more than two months before the travel date) and sending multiple emails, we were unable to determine the cause of the problem. The Madrid embassy disclaims responsibility for the electronic visa and refers applicants to the Nigerian Immigration Services in Abuja.
On the day of departure, two team members still did not have their visas, which forced us to go to the Madrid embassy on the same day as the flight to seek a solution. Thanks to Jasper Suleiman (an embassy employee) and the ambassador’s secretary, we obtained the visas barely three hours before departure.

For all these reasons, we recommend that teams for future campaigns carefully complete the visa application with the exact passport details and thoroughly review the emails received, including spam folders, ensuring that the acceptance or denial document is received. The process should be started with sufficient time to address potential issues, but not earlier than three months in advance, which is the validity period of the visa.
We also discussed the visa difficulties with Austin Ella, who assured us that for future campaigns he will try to have a contact within the Immigration Services to expedite the process.
Furthermore, we agreed with him that, for future campaigns and in order to avoid legal issues, team members should be registered with the Medical Council, the body responsible for regulating physicians and ensuring good medical practice in Nigeria. This is a procedure that must be carried out by local staff, and in the last two campaigns no such registration had been completed, leaving all responsibility with Dr. Thaddeus, the physician at Bishop Murray Medical Center.
On the day of our arrival at the airport, Dr. Thaddeus met us at the baggage claim area and assisted us with customs clearance. This is always a critical step since, although on this occasion we carried anesthetic medication with an export report from the Spanish Agency of Medicines, luggage is often inspected in an attempt to demand money.
This time we encountered difficulties due to material that was close to expiration or already expired (upon entry they require expiration dates of more than six months, which is reasonable). Thanks to Dr. Thaddeus’s mediation and after a payment of approximately €120, we were able to bring everything in.
SURGICAL PROCEDURES (Annex 1)
Two weeks after our return, we contacted Dr. Thaddeus, who informed us that he had not received any complicated patients.
- CAMPAIGN REPORT
3.1. LOCATION
Nigeria is a West African country bordered by Niger to the north, Chad to the northeast, Cameroon to the east, and Benin to the west. Its southern coast lies on the Gulf of Guinea in the Atlantic Ocean. The federation comprises thirty-six states and the Federal Capital Territory, where the capital, Abuja, is located.
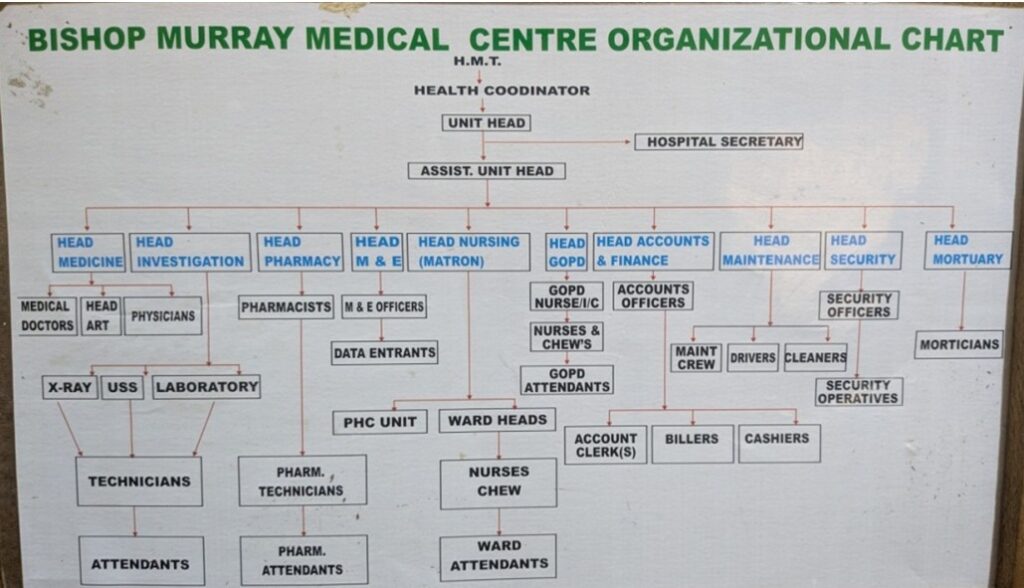
The Bishop Murray Medical Center is a hospital located in Makurdi, about 300 km southeast of the capital (almost six hours by bus). It is a healthcare center belonging to the Catholic Diocese of Makurdi. It is a simple but well-equipped center with radiology services, operating rooms, laboratory, sterilization, etc. It has several inpatient wards separated by gender and some private rooms without nursing services.
We stayed in a diocesan residence free of charge, in single rooms with air conditioning and private bathrooms—simple but adequate. The hospital is about a 15-minute drive from the residence.
3.2. TEAM
Coordinator: Sebastián Fernández Arias
Nurses: Estela Sala Carbellido, Pilar García Diez
Anesthesiologists: Maribel Real Navacerrada, Paula Alejandra Morales, Antonio Hinojosa Jiménez
Endocrine Surgeon: Enric Caubet
General Surgeons: Lucia Catot Alemany, Elisabet Julia Verdaguer, Elisabeth Redondo Villahoz
Pediatric Surgeon: Valeria Solari
Pediatrician: Johanna Würzl
Support Staff: Gloria Hospedales i Catot, Salifou Hankouraou
3.3. LOCAL STAFF
Our contact in Nigeria was Dr. Austin Ella, who acted as our liaison with the Diocese to coordinate all pre-departure arrangements. The Medical Director of Bishop Murray Medical Center was Father Peter Paleve, who looked after us throughout the campaign.
In Makurdi we were accompanied by Dr. Thaddeus, a general practitioner with surgical knowledge, with whom we addressed issues related to equipment, patients, etc. He was also responsible for patient selection and for organizing the daily surgical schedules. Although there were enough patients to fill the daily workload, it is advisable to agree in advance on the expected activity, since in our case approximately 50 thyroid surgeries were scheduled over six days, which proved unfeasible, and on the last day there were no pediatric patients.
During the working week we collaborated with Jacob, Nicholas, Timothy, and Joshep, who were responsible for patient transport and worked efficiently and tirelessly.
Similarly, Bridget, Charity, and Josephine were in charge of sterilization to ensure all material was ready, and Benedicta assisted our anesthesia team.
3.4. EQUIPMENT
The Bishop Murray Medical Center is well equipped and has the necessary resources to carry out a campaign involving procedures under spinal and general anesthesia.
The surgical area consists of a large room that allows the installation of several operating tables simultaneously, separated by screens. It has air conditioning and an electrical supply with generator support, although surgical lighting is limited, making the use of headlamps necessary for some procedures.
The hospital has two electrosurgical generators, one of which required repair during the campaign. The team provided two additional generators (one from the Foundation and one from Dr. Catot), which allowed simultaneous work on four tables.
It also has a Dräger ventilator with a Philips monitor, which made it possible to perform procedures under general anesthesia (additional anesthesia-related information is provided below).
The Radiology Service has an older ultrasound machine, which Dr. Caubet used to assess all patients scheduled for goiter surgery.
The team provided pulse oximeters and a portable blood pressure monitor, which proved useful during the campaign. The hospital did not have these devices, and they were left there at the end of the campaign.
3.5. ANESTHESIA
3.5.1. Operating Area and Recovery
Within the surgical area, the center has a Dräger Atlan 300 anesthesia machine with a Dräger Vista 120 monitor, including gas monitoring and capnography, as well as two basic monitors (pulse oximetry and non-invasive blood pressure).
There is no structured post-anesthesia care unit, so an area adjacent to the operating room was designated for postoperative monitoring, especially for patients undergoing thyroid surgery. In this context, the finger pulse oximeters and portable blood pressure monitor provided by the team were extremely useful.
3.5.2. Anesthetic Techniques
During the campaign, general anesthesia, spinal anesthesia, and sedation techniques were used, adapted to the pathology and available resources.
Pediatric anesthesia was performed using inhalational anesthesia with a laryngeal mask under spontaneous ventilation, combined with regional blocks, using a sevoflurane vaporizer and a Mapleson-type ventilation system provided by the team, with oxygen supplied via cylinders. The high gas consumption required local purchase of sevoflurane at a high cost.

In thyroid surgery, the Dräger Atlan 300 ventilator allowed safe general anesthesia, although without the availability of medical air. Anesthetic maintenance with propofol was possible thanks to the intravenous infusion pump provided by the team. Given the nature of the pathology, it is strongly recommended to bring a videolaryngoscope, which allowed resolution of two difficult airway cases using a King Vision device and a Frova-type guide.
One episode of severe bronchospasm was recorded, which responded to standard treatment. Postoperative cervical hematomas were drained under sedation. Ketamine proved particularly useful in this setting.
For adult abdominal wall surgery, spinal anesthesia was used without significant incidents. At one operating table, monitoring equipment provided by the team was required.
Due to a strike at the other hospital in the city, unforeseen emergency cases were treated, including cesarean sections, ectopic pregnancies, a uterine rupture, and a perforated appendicitis. Cesarean sections and ectopic pregnancies were performed under spinal anesthesia; more severe cases required general anesthesia with orotracheal intubation. The patient with uterine rupture required advanced cardiopulmonary resuscitation, central venous access, and whole blood transfusion, evolving favorably despite the absence of an ICU at the center.
This experience highlights the importance of bringing emergency equipment and medication, which on this occasion could be partially obtained from previous campaigns.
3.5.3. Materials
During the campaign, local resources and materials provided by the Foundation and by team members were used.
A need was identified for future campaigns to have a larger supply of tranexamic acid, antihypertensive drugs (especially labetalol), opioids such as fentanyl—very difficult to obtain locally—as well as a greater number of three-way stopcocks and extension lines.
The usefulness of materials from previous campaigns was confirmed. At the end of the mission, medical supplies and medications were left under proper custody with a detailed inventory.
3.5.4. Training Impact and Knowledge Transfer
Given the absence of formally trained anesthesiologists, practical training was provided to Benedicta, the nurse responsible for anesthesia, in airway management techniques (including videolaryngoscope-guided intubation with an Airtraq-type device), general anesthesia, and pediatric anesthesia. Practical teaching was also provided to nursing staff and nursing students to assist in pediatric surgical procedures.
3.6. ASEPSIS AND SURGICAL MATERIAL
The sterilization room adjacent to the operating theater has two or three pressure-cooker-type autoclaves in which all material was sterilized. We brought surgical material from the Foundation distributed in six boxes (two for thyroid surgery and four for hernias), which were sterilized in small cloths. Before starting the campaign, all material was labeled. Dr. Solari also brought pediatric surgical instruments.
The main limitation encountered was with surgical gowns, as we did not bring enough for the entire campaign (they take up a lot of space and are not easy to obtain). As a result, we had to use cloth gowns from the hospital and re-sterilize some of the gowns we had brought.


We established a basic set for a standard hernia procedure, which was used for most of the interventions, consisting of:
- Sterile gloves for the team and gowns
- Antibiotic
- Antiseptic
- Scalpel blade
- Syringe for local anesthesia
- Large sterile drape (150 x 180 cm) for the patient
- Small sterile drape (50 x 50 cm) for the table
- Mesh
- Electrosurgical unit
- Sutures (PDS 2/0 x 2 for the mesh and Monocryl 3/0 triangular needle for the skin)
3.7 DAILY LIFE IN MAKURDI
On the day of our arrival at Abuja airport, Dr. Thaddeus met us at the baggage claim area and assisted us with customs. Dr. Austin Ella was waiting for us in the parking area. We traveled by bus to Makurdi without any incidents.

On Saturday, the day of our arrival, we were welcomed at Bishop Murray Hospital with a welcoming ceremony where we met all the hospital staff. That same day we took the opportunity to organize and store all the material.
On Sunday, we were welcomed again at the diocesan mass early in the morning, and from there we went to the hospital to begin the surgeries.During our stay in Makurdi, we stayed at the diocesan residence about 15 minutes by car from the hospital. We usually met in the dining room around 6:45–7:00 a.m. for breakfast (coffee with scrambled eggs or pancakes), and at 7:30 a.m. we were picked up to go to the hospital to begin the surgeries.


The typical day consisted of reviewing patients operated on the previous day and assessing those scheduled for surgery that day. The surgical day usually started around 9:00 a.m. and ended around 8:00 p.m. We stopped for lunch between 1:00 and 2:00 p.m., although most of the time we ate in groups depending on the surgical schedule. At the end of the day, we were picked up again from the hospital and finished the day with dinner together in the residence dining room.
On the last working day, during lunchtime, a farewell ceremony was held and we were presented with honorary garments as gifts.


Outside the hospital there were not many leisure options, or at least none were recommended to us. On the last day, while part of the group organized the remaining material and packed all the equipment we were bringing back (a list of materials left behind is included in Annex 2), another part visited a local market and made some purchases (mainly fabrics).

We left Makurdi the day before our return flight and stayed the last night in Abuja, in a diocesan residence similar to the one in Makurdi and very close to the airport (about 20 minutes away). As we had incurred some unforeseen expenses during the campaign (some medications and airport “fees”), it was agreed that the hospital would cover the accommodation in Abuja, so there was no cost to us. We had dinner at the residence and left for the airport at 6:00 a.m. the following day.
The return trip proceeded without incident, and in London we said our goodbyes and continued on to our respective destinations.
3.8. TOTAL COST OF THE CAMPAIGN
Estimated total cost: €17,831.40 / 13 people* = €1,371.65 per person.
*Estimated expenses related to the 13 team members from Spain and Austria.
Flights: (Vienna €972.35, Barcelona €1,033.73, Madrid €1,056.15). Total: €12,416.52
Insurance: €48.50 (price from Spain**) ≈ €630.50
**Ten people purchased insurance through an agency; one traveling from Spain and the two from Vienna purchased it independently. It is estimated that the cost was the same for all 13 people for calculation purposes.
Visas: €256 x 13 = €3,328
Bus transport between Abuja and Makurdi: €1,106.38
Additional expenses: approximately €350 (airport “fee” for materials €120 + purchase of Sevoflurane)
ANNEX 1
SURGICAL PROCEDURES
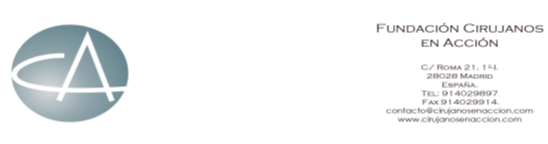
Total procedures: 129
Total patients: 116
Adults:
- Inguinal hernia: 39
- Bilateral inguinal hernia: 5
- Epigastric hernias: 3
- Incisional hernias: 2
- Lipomas: 4
- Hydrocele: 6
Pediatric:
- Inguinal hernias: 20
- Bilateral inguinal hernias: 4
- Umbilical hernia: 3
- Lipoma: 1
- Thyroglossal duct cyst: 1
- Hydrocele: 4
- Cryptorchidism: 1
Endocrine Surgery:
- Bilateral subtotal thyroidectomy: 9
- Hemithyroidectomy: 16
- Isthmic tumorectomy: 2
- Hematoma aspiration: 3
Additional:
- Cesarean sections: 4
- Ectopic pregnancies: 2
- Uterine rupture: 1
- Appendectomy: 1
Complications:
- Post-thyroidectomy hematomas: 3
ANNEX 2
INVENTORY OF MATERIAL LEFT AT THE HOSPITAL
- Gloves size 7.5: 50 units
- Disposable sterile forceps (14.5 cm): 8 units
- Dressings: Various
- Mepilex (silicone dressings 10 x 18 cm): 20 units
- Surgical drapes:
- 100 x 80 cm: 15 units
- 150 x 180 cm: 10 units
- Fenestrated (75 x 90 cm): 8 units
- Argenpal (skin stick): 5 containers
- Electrosurgical pencil tips: 20 units
- Fluid controller (flow regulator): 12 units
- Peripheral IV dressings: 300 units
- Mefix 20 cm x 10 m: 3 units
- Scalpel blades: No. 11 (200 units), No. 15 (50 units), No. 23 (250 units)
Spanish Team in Freetown, Sierra Leone, 13-24 Nov 2025
SURGICAL CAMPAIGN AT KINGTOM POLICE HOSPITAL IN FREETOWN, SIERRA LEONE.
DATE: 14-23 NOVEMBER 2025
The team began to form in April and was complete in June with 11 people (anaesthesia, nursing, general surgery and paediatric surgery). The campaign took place between 14 and 23 November.
DOCUMENTATION AND VISAS:
To travel to Sierra Leone, the only mandatory documentation is a valid passport, with a minimum validity of 6 months from the date of entry, a visa and a yellow fever vaccination certificate.
The visa is an electronic visa (E-Visa) that is very easy to obtain. You just have to apply online (https://www.evisa.sl/#/home) and pay the fee (84.27 USD, 80 for the visa and 4.27 for processing costs). The yellow fever vaccination certificate is an official certificate that is obtained after receiving the vaccine and paying a fee (currently €19.46). It is advisable to visit one of the authorised international vaccination centres at least one month before departure. A list of these centres can be found on the Ministry of Health website (https://www.sanidad.gob.es/areas/sanidadExterior/laSaludTambienViaja/centrosVacunacionInternacio nal/centrosvacu.htm).
In addition, it is advisable to take out travel insurance and professional liability insurance. The Foundation for International Cooperation of the Medical Association (https://www.fcomci.com) offers liability and travel insurance for registered doctors who are listed in the national register of cooperating doctors of that organisation. Some nursing associations, such as the one in Madrid, have taken out civil liability insurance for their members that includes humanitarian aid activities. Some individually taken out insurance policies can also be temporarily extended to cover international cooperation abroad.
In addition, a series of documents must be processed for temporary work permits in Sierra Leone, which are: a certified translation into English of the degree (bachelor’s degree or specialisation for doctors and diploma/degree for nurses), a summary CV in English, a certificate of professional suitability/certificate of good conduct (which can be requested from the official associations), and a registration form for the Medical and Dental Council of Sierra Leone (the latter only for doctors). Apart from the cost of the certified translation, if you do not already have one, and the fee for the certificate of professional suitability charged by some professional associations, the procedure is free of charge.
TRANSPORT:

The flights were arranged from Madrid with the help of Angelis González, a freelance travel agent with Halcón Viajes, which has been collaborating with the Cirujanos en Acción Foundation for years.
The five team members who came from outside Madrid (one from Segovia, one from Menorca, one from Murcia and two from Lleida) arranged their own travel to Madrid.
The team travelled on Thursday, 13 November 2025, at 7:00 p.m. from Madrid to Freetown with a three-hour stopover in Casablanca, arriving at Lungi Airport in Freetown on 14 November 2025 at 3:35 a.m.
The return journey took place on Sunday 23/11/2025 at 6:50 a.m., with the trip beginning at 2:00 a.m. to reach the airport by ferry. There was also a stopover, this time of two hours, in Casablanca, arriving in Madrid at 3:30 p.m.
These flights with Royal Air Maroc were chosen because they allowed us to travel more quickly and their dates were more convenient for the campaign, despite some bad experiences with lost luggage.
Indeed, five of the packages did not arrive in Freetown initially. After filing the corresponding claims at Lungi Airport and taking the necessary steps, both by Dr Konteh from Sierra Leone and by Angelis González and David Luengas from Madrid, three of the five lost packages were located and arrived in Freetown on 21 November (the last day of the campaign). The other two packages arrived, without prior notice, on 27 November, when the team was already back in Spain. It was agreed with John Konteh that they would be kept for the next campaign, which will take place in January.
For internal transport, airport police personnel were waiting for us on arrival to help us speed up border formalities and, once through customs, we were met by Dr John Konteh, Deputy Director and Medical Superintendent of the Sierra Leone Police Medical Services, who was our contact person prior to arrival to organize everything necessary. He accompanied us to take the Seacoach Express.
This is a ferry that connects the airport (located in Lungi Town) with the Freetown peninsula, and is the fastest way to get there, as ground transportation involves a 3-hour trip around Tagrin Bay. The price is
$45 per person per trip and includes the shuttle bus from the airport to the ferry terminal (about 5-10 minutes) and the ferry ride, which takes about 45 minutes.
From the Freetown ferry terminal, we travelled to the hotel in a Toyota Coaster minibus with official police registration plates, which took us daily from the hotel to the hospital and back.
We also used it for the trips we made on our last day, which was a day off.
TRANSFER OF MATERIAL:
A total of 22 pieces of checked luggage weighing between 18 and 23 kg were transported, containing surgical and anaesthetic equipment, including two anaesthesia monitors loaned to one of the anaesthetists (Celia Garrido) and two electric scalpel generators belonging to the foundation.
The team was responsible for obtaining the necessary materials for the campaign.
The 12 de Octubre Hospital in Madrid donated anaesthetic medication worth €750, arranged by anaesthetist Javier Silva.
We also received a donation of sutures worth €1,000 from B Braun, arranged by paediatric surgeon Rocío Gutiérrez.
A fellow general surgeon from 12 de Octubre Hospital, Alfredo Vivas, who did not attend the campaign but wanted to collaborate, made a personal donation of 25 boxes of 40 1g paracetamol tablets and 15 200ml bottles of ibuprofen syrup (20mg/ml), enough to provide post-operative analgesia for all patients who underwent surgery.
The surgical meshes used were fragments of polypropylene meshes cut under sterile conditions and subsequently re-sterilized at the 12 de Octubre Hospital.
The rest of the material (surgical gowns, sterile cloths, gauze, compresses, sutures, dressings, gloves, antiseptic solutions, electric scalpel terminals and plates, scalpel blades, anaesthetic medication, syringes, needles, IV lines, etc.) were obtained as part of small donations from the hospitals where all the participants work, and some material was also taken from the warehouse of the Cirujanos en Acción foundation.
ACCOMMODATION:
As in previous campaigns, we stayed at the Jam Lodge Hotel. The hotel is quiet and offers single or double rooms with private bathrooms and breakfast included in the price. It is also located about 10-15 minutes from the hospital, which makes it convenient for starting and ending the day. As with the last group in September, we made the reservation through Booking, as it was cheaper than booking directly with the hotel. And thanks to the Genius discounts of one of the team members (Nacho Ortega), who made all the reservations, we got a discount of up to 32% off the original price, so the price for 8 nights for single rooms was £375.12 and for double rooms £515.92. To that we had to add a total of £70 per room to be allowed to check in early on the day of arrival (we arrived around 7:30 a.m. and check-in time is 3:00 p.m.) and a late check-out on the day of departure (we kept the room until 7:30 p.m.).

ADULT PATIENTS
A total of 137 procedures were performed on 116 patients.
PEDIATRIC PATIENTS
A total of 62 procedures were performed on 57 patients.
According to local staff, no complications were reported either during the campaign or afterwards.
1. CAMPAIGN REPORT
2.1. THE LOCATION
Freetown, the capital of Sierra Leone, is a destination where the Cirujanos en Acción Foundation has established ties since 2019, when the first surgical campaign was carried out in this city in this West African country.
The health center where the campaign took place was the Kingtom Police Hospital in Freetown, a facility belonging to the police force, an institution with considerable influence and power throughout the country. In the past, this hospital only treated members of the police force and their families, but in recent years it has extended its medical services to the entire population of the area.
The hospital consists of several modules for emergency care, basic primary care, obstetrics consultations, etc.
The module where the surgical block is located has two floors. On the upper floor, there are several hospital rooms, offices, and consultation rooms.
It has a basic laboratory (simple blood counts and biochemistry, basic urine analysis and rapid tests for various pathologies, including HIV).
The surgical area is located on the ground floor. It has two operating theatres (one large and one small), separated by the sterilization room with an autoclave and a small room with a sink, all connected.

Adjacent to the large operating theatre is a small room with a table where we were brought coffee and fruit and ate lunch. Adjacent to the small operating theatre is a room with cupboards and a bathroom that we used to store the equipment we brought with us. On the first floor, we were given another room with a bathroom and a key, which we used as a changing room and to leave our personal belongings.
Both operating theatres have air conditioning, although it did not always work properly.

Outside the surgical area on the same floor, there are three hospital rooms that were used during the campaign for surgical patients (one for men, one for women and one for children).
There are also two offices (one of them belonging to John Konteh) that we use as consultation rooms on the first day to carry out triage.
2.2. THE TEAM
Our team consisted of a total of 11 volunteers:
- Nursing: Carlota Castillo Sainz, Assumpta Ferrer Benejam and Laia Ribelles Moreno.
- Paediatric Surgery: Rocío Soledad Gutiérrez and Detlef Oliu San Miguel.
- General Surgery: Sandra del Barrio Anaya, Marta Gutiérrez Andreu, Ignacio Ortega Fernández and Daniel Pastor Altaba (team leader).
- Anaesthesia: Celia Garrido Yuste and Javier Silva García.
2.3. LOCAL STAFF

Dr John Konteh, Deputy Director and Medical Superintendent of the Sierra Leone Police Medical Services, is, as mentioned above, the contact person responsible for coordinating the campaign with us. He is a highly experienced endocrinologist who trained in London, which enables him to understand our point of view very easily. He is responsible for organizing all local transport and making preliminary calls to patients for the campaign, based on what has been agreed (in our case, we agreed that we would perform paediatric and adult surgery, but not endocrine surgery, and he was responsible for gathering more than 400 patients who were candidates for surgery).
Although he was not present in the surgical area, he was present at the hospital on many occasions and available by telephone at all times.
In addition, we had the enormous support of David Fanday, the hospital’s nursing administrator, who was always looking out for us and accompanied us on our trips from the hotel to the hospital and vice versa. Furthermore, given that five of the packages were missing, and that one of them contained almost half of the anaesthetic medication and all of the spinal anaesthesia needles, we had to obtain supplies locally in order to carry out the campaign. Thanks to David and Dr Konteh, we were able to obtain everything we needed on a daily basis to continue with the surgical activity. It was thanks to them and the enormous adaptability of the anaesthetists, especially Javier Silva, who was in charge of the two adult tables, that the campaign was able to go ahead.
However, we must also mention and thank the rest of the staff who were present and collaborating during the long surgical days (Mohamed Sorie Kamara, Unisa Sesay, Francis Raymond Kamara, Mary T. Musa, Bintu Jimmisa, Davida Dumbuya, Fatmata Kabba, Francis S. Conteh, Philipp Kpange…), the nursing staff who were responsible for calling the patients who had to come in each day, preparing them before surgery, caring for them in the immediate post-operative period, collaborating with us in the operations and being in charge of cleaning and re-sterilizing materials.

On some days, we had the help of Sia, an anaesthesia technician who works at the Italian hospital but who came to help with the campaign at the Police Hospital when he was available.
We were also accompanied by some nursing students (Sheriff, Ibrahim, Konneh…) who were very committed and eager to learn.
2.4. EQUIPMENT
The hospital has acceptable surgical equipment for minor surgeries (inguinal hernias, soft tissue tumors, small ventral hernias, etc.), which is the type of surgery we perform. Some of the equipment is already very worn (Kocher clamps that do not close properly or needle holders that do not grip the needle well, for example), but it can still be used for these types of procedures. There is enough to prepare several boxes with two toothed forceps, two non-toothed forceps, needle holders, mosquito forceps, Kocher forceps, scissors and retractors, and to re-sterilize without having to wait. For more complex or delicate surgery such as thyroidectomies, I think it is advisable to bring your own equipment. In our case, Rocío Gutiérrez, a paediatric surgeon, brought a couple of boxes of instruments that were used for paediatric cases.
There is an electric scalpel that also works “acceptably” (increasing the power significantly to be able to coagulate), with a metal plate but compatible with the adhesive plates we normally use here, and with a three-prong connector for the button terminal. We brought two more generators, so we had one per table. In Sierra Leone, the mains voltage is 230V and the frequency is 50Hz, and the power socket is type G (British). It is important to remember to bring adapters so that the earth connection works properly. As for consumables, it is best to bring them from Spain. However, since five of our packages were lost and we only recovered three on the last day, we ran out of gowns and gauze during the last few days.
There are cloth gowns that can be re-sterilized, and gauze can also be obtained there.

As for lighting, there are only two large lights, one of which broke on the first day and could not be repaired while we were there. There are a couple of smaller lights that are not very mobile and are completely insufficient. Therefore, a good-quality head torch is essential (torches with built-in batteries tend to give off little light. It is better to use one with replaceable batteries, which are usually more powerful and also allow you to have spare batteries, as surgical procedures are long and the batteries start to fail in the last few hours, when the light is most needed).
2.5. ANAESTHESIA
There is currently a Dräger Atlan ventilator with Isoflurane and Sevoflurane vaporizers (donated by the Bisturí Solidario foundation) installed in the larger operating theatre. The installation consists of an oxygen connection connected via a tube to a replaceable O2 cylinder and a medical air generator to mix the gases. The dependence on an oxygen cylinder limits the use of high flows and inhalation inductions, as it is consumed at a faster rate, but most paediatric patients had an intravenous line, which allowed for intravenous inductions.

Our initial intention was to use the smaller operating theatre for paediatric patients and the larger one for two adult tables. However, although it would have been feasible to move the anaesthesia machine, as the only “fixed” element is the oxygen hose, which is anchored to the wall with clamps, we did not risk moving the ventilator, which had caused problems in previous campaigns and was working well in our campaign. Therefore, we set up one paediatric table and one adult table in the large operating theatre and another adult table in the small one.
There is another ventilator outside the operating theatre that had previously been working but was awaiting repair.
There are also three oxygen concentrators, although only two were working and at times they had problems due to power failures.
The anaesthesia machine has a multi-parameter monitor, but some of the measurements were not available, so it was necessary to supplement it with portable pulse oximeters. The machine’s ventilator has capnography. Each adult table has a Phillips mp monitor that allows complete monitoring, although at times it was necessary to use them on battery power due to the limited number of working sockets, which meant that they shut down at certain times. One of them had a problem measuring blood pressure. In these cases, a portable blood pressure monitor owned by the hospital and small portable pulse oximeters carried by the team were used.
Adults:
As there was only one anaesthesia machine in operation, it was used for paediatric patients, and almost all adults underwent spinal or local anaesthesia combined with more or less deep sedation when necessary, mainly combining propofol and ketamine in spontaneous breathing with nasal cannulas and, in some cases, clearing the airway with Guedel-type cannulas when deeper anaesthesia was required. In this regard, it should be noted that the soft tissue injuries were large, and almost all required moderate to deep sedation given the limitation in achieving an adequate level of anaesthesia using only local anaesthesia.
It should also be noted that the performance of intrathecal anaesthesia was conditioned by the lack of intrathecal needles due to the loss of luggage, so different models from other campaigns and those that could be obtained from the hospital were used. From an anatomical point of view, ligaments in general are highly resistant, and the dosage tends to be higher given the younger age of the population and greater body size compared to our population (doses between 13-17 mg of hyperbaric bupivacaine depending on the location of the intervention area), with adequate tolerance.
Haemodynamics. On the first day, we observed a lack of effect from the hyperbaric bupivacaine used, which was resolved by changing batches, without being able to establish the cause. We do not know whether temperature changes during transport can alter the medication. Given the limited supplies, the packaging of sterile gloves was used as a sterile field for the intradural technique, and cloths were not used to delimit the puncture field, replacing it with extensive cleaning of the entire back and hips with alcoholic chlorhexidine. In general, local anaesthesia was not administered prior to intradural puncture for the same reason, so punctures were generally performed with intradural needles without an introducer.
Locally, intravenous catheters with ports for administering medication, infusion lines, and 0.9% saline solution are available without restrictions, which allowed all patients to be hydrated before the intradural procedure. It should be noted that patients undergo prolonged fasting and that heat and humidity are significant factors. The lines were cannulated by local staff before transfer to the operating theatre, but it is advisable to check them thoroughly before use, as a percentage of them were extravasated.
Only one case was performed under general anaesthesia, which had been impossible to anaesthetise regionally a few days earlier and was rescheduled for the last day when the paediatric cases were completed. No allergic reactions were recorded, only four patients presented hypotension after anaesthetic induction, which was resolved with the timely administration of ephedrine, and one episode of vasovagal presyncope due to pain during a procedure under local anaesthesia, which was resolved with atropine and conversion to deep sedation. Once again, we emphasize the importance of monitoring and administering anxiolysis and/or sedation in procedures proposed for local anaesthesia.
Paediatrics:
All procedures were performed under general anaesthesia with a laryngeal mask, either with sevoflurane (a vaporizer and limited supply of the agent are available) or with intravenous bolus maintenance (no infusion pump is available). The use of inhalation anaesthesia is limited by the consumption generated by the inability to perform low flows and by the consumption of oxygen cylinders. In some cases where the oxygen cylinder was depleted during the procedure, it was necessary to switch to an oxygen concentrator via a Mapleson mask in spontaneous ventilation. All paediatric patients received local anaesthesia to reduce anaesthetic requirements given the lack of fentanyl and limited ketamine due to lost luggage.
Most of the children had a venous line prior to the procedure, which facilitated intravenous induction. There was only one case of severe laryngospasm/bronchospasm and loss of venous access with difficulty in recanalization.
To be taken into account in the next campaign, the suitcase that arrived later contained numerous intrathecal needles, most of which have an NRFit connection, requiring syringes with the same connection, which are transported in the same package. This limits the use of these syringes for intravenous drugs and vice versa, so we recommend bringing a large supply of syringes for administering medication, as there are no infusion pumps either.
2.6. ASEPTIC TECHNIQUES AND SURGICAL EQUIPMENT
There is a steam autoclave that allows the material to be re-sterilized (in metal trays and double cloth). Gowns, cloths and gauze can also be sterilized. We also re-sterilize electric scalpel tips, which generally last for 2-3 uses before eventually ceasing to function. The local staff carry out the cleaning and re- sterilization tasks very efficiently and we had no problems in this regard.
2.7. OUR LIFE IN FREETOWN
We arrived at Freetown International Airport in Lungi Town on Friday, 14 November 2025, at 4:30 a.m. After retrieving the 17 pieces of luggage (out of a total of 22 checked) that had arrived and filing the corresponding claims for the lost luggage, we passed through customs. John Konteh met us in the arrivals area, and together we took the ferry and then the minibus to the hotel, arriving between 7:30 and 8:00 am.
After resting for a few hours, at 12 noon we were picked up and taken to the hospital, where we were greeted by the local team and hundreds of patients waiting to be triaged.
After opening the packages that had arrived, to get an idea of what was missing and what we could start operating on in the first few days, the surgeons began to consult with the patients while anaesthetists and nurses set up the equipment and organized the operating theatre area. After triaging some 230 patients and informing them that not all of them could probably be operated on, we decided to stop, even though there were still more than 100 patients waiting.
That day we had dinner at the hotel (we had ordered dinner in advance) for $15 per person. From Saturday 15/11/2025 to Friday 21/11/2025 we performed surgical procedures.
We had breakfast every day at the hotel around 7:00 a.m., and at 7:30 a.m. David, Abu (John Konteh’s personal bodyguard who accompanied us the entire time), and the driver picked us up in the bus. The trip to the hospital took about 10-15 minutes (depending on traffic, although we were often escorted by a police motorcycle that cleared the traffic ahead of us).
We started work at around 8:00 a.m. While the surgeons checked on the patients who had undergone surgery the previous day, the rest of us organized the operating theatres to begin surgical activity, with three tables (two for adults and one for children). Between 2:30 and 3:00 p.m., we all took a break to eat. The first few days, they brought us fruit and bread, and we ate cold cuts that we had brought from Spain, but the last few days we ordered local food (for 50 leones per person (less than 2 euros), they brought us rice with potato leaves or cassava and meat or fish. We also had fried plantains if we ordered them first thing in the morning (paying for them separately). There isn’t much variety, but it’s local food, and although it can get tiresome if you have it every day, it’s fine for a few days.

Then we continued until we finished with the patients scheduled for the day. We usually finished between 8:00 p.m. and 9:00 p.m.
For dinner, we only ordered dinner at the hotel on the first day. The rest of the days, we ordered dinner from a restaurant near the hotel and the hospital (with the help of David, who was always available) and picked it up on the way back to the hotel at the end of the day (chicken, salads, meat, pizza). Several days we decided to eat directly at the restaurant, inviting David, Abu, and the driver.
On Monday, 17 November 2025, we started a little later because, as every year, we were received first thing in the morning by the Inspector General of the Sierra Leone Police (Mr. William Faya Sellu) at a formal ceremony in which both he and Dr. John Konteh thanked the team and Cirujanos en Acción for their work at the Police Hospital in recent years, and we were given our temporary work permits.
On the last day of work, Friday 21/11/2025, we finished early in the afternoon so that we could rest a little more that day.
On Saturday, 22 November 2025, we took the day off. In the morning, we visited the Tacugama chimpanzee sanctuary, which is about 40 minutes from the hotel (we had the police bus and the company of David and Abu for transport on this day). This center is responsible for rehabilitating rescued chimpanzees (most of which had been sold as pets) so that they can return to their natural environment. The visit costs 350 leones (about £13) and lasts approximately one hour.

Then we visited the Cotton Tree (national symbol) and a craft market.
After resting for a while at the hotel, we were picked up at around 7:00 p.m., with all our luggage, to go to the official farewell dinner with the hospital staff, where we were also given some gifts. After dinner and a few hours of partying, we went straight to the ferry terminal to catch the ferry to the airport and catch our flight on Sunday 23/11/2025 at 6:50 am.
2. CONCLUSION
2.1 Strengths of this place:
The hospital’s appeal is so great that patients from neighbor countries have also been attending recent campaigns, which helps Cirujanos en Acción reach a larger number of people. Working hand in hand with the police makes any kind of administrative task much easier (there were no problems at customs on arrival despite transporting large quantities of surgical equipment and medicines, we were not stopped at any roadblocks and even during peak traffic hours we got through without any problems). Furthermore, as the campaign is in Freetown, there is no need for long internal journeys after arrival. Another advantage is that, in cases of lost luggage, as happened to us, it has been possible to obtain replacement materials (which would have been much more difficult, if not impossible, had we been in a more isolated area).
The local team has always been very involved and helpful at all times. They also take advantage of the campaigns to bring in nursing students as a training opportunity.
All of this has made for a very pleasant working environment.
3.2. Areas for improvement:
Although conditions in the surgical area have improved over time (new fan, air conditioning in almost all rooms, adequate sterilization capacity, etc.), there are still areas for improvement. The lights are not of good quality and are insufficient for the three tables, making a head torch essential for safe operation. The surgical equipment, although sufficient in quantity for minor surgeries, is not of very good quality. The operating tables are also old and sometimes do not maintain their position (the height gradually lowers).
The ventilator, although new, is connected to an oxygen cylinder, which prevents it from being used to its full capacity.
It would also be useful to have another ventilator in the second operating theatre.
Nevertheless, this hospital more than meets the expectations for surgical campaigns, and conditions will likely continue to improve over time.
3. BUDGET: (brief breakdown of expenses)
4.1. COST PER PARTICIPANT:
Flights: €1,085
Visa: 84.27 USDà 72 euros Luggage transport (packaging): €20
Ferry: 70 USD (35 per trip)à 60 euros
Accommodation: USD 670 double room (335 per person). USD 530 single room (average of USD 450 USD)à572 euros double (286 per person), 452 euros single (average, 361.5 euros) Meals (lunch, dinner and beers): 104.53 euros
Total price per person: Between €1,630 and €1,795 per person approximately (depending on whether you share a room or not).
4.2. TOTAL COST OF THE CAMPAIGN:
Total cost for the 11 participants, including flights, visas, transport, accommodation and living expenses:
€18,755 in total.
4. SIGNATURES
Signed on behalf of the entire team: Daniel Pastor Altaba, team leader. Surgeons in Action
PASTOR ALTABA
Aus-Bulg Team to Mongolia. May 2025
REPORT ON THE INTERNATIONAL TRAINING “MODERN TRENDS IN SURGICAL TREATMENTS OF HERNIAS”
2025.11.25
1. Introduction
In accordance with the long-standing cooperation agreement between the Second State Central Hospital and the Hernia International Organization, the international on-site training titled “Modern Trends in Surgical Treatment of Hernias” was successfully organized for the 12th consecutive year. The training took place from May 26–31, 2025 at Darkhan-Uul Provincial General Hospital, and from June 2–7, 2025 at the Second State Central Hospital.
2. Participants
Mongolian Team
• Ts. Narmandakh – Honored Doctor of Mongolia; Chair of Surgical Council, Second State Central Hospital; Consultant Surgeon at the General Surgery Center; Master of Medical Science; Clinical Professor (Team Leader)
• Z. Sonor – Colorectal Surgeon, General Surgery Department, Second State Central Hospital; Master of Medical Science
• G. Gerelmaa – Resident Doctor, General Surgery Department, Second State Central Hospital
• D. Batdorj – Resident Doctor, General Surgery Department, Second State Central Hospital
International Volunteer Surgeons (Hernia International Organization)
• Robert Dudley Bohmer (MD, Consultant Surgeon) – Australia
• Hairul Anuar Ahmad (Ph.D, Consultant Surgeon) – Australia
• Dragomir Danailov Dardanov (Ph.D, Consultant Surgeon) – Bulgaria
• Zheng Andrew Zhang (MD, General Surgeon) – Australia
3. Training Attendance
A total of 92 participants — surgeons, residents, trainee doctors and nurses — attended the program. Participants represented public and private healthcare organizations from:
Darkhan-Uul, Orkhon, Govisümber provinces, and Sükhbaatar, Nalaikh, Baganuur, Bayanzurkh, Chingeltei, Songinokhairkhan districts.
4. Training Content and Academic Activities
In addition to the practical workplace-based sessions, theoretical lectures were conducted during and after surgeries in classroom format. Participants received detailed explanations and responses to their questions from the surgical instructors.
During this period, Dr. Hairul Anuar Ahmad also visited the Mongolia–Japan Hospital of the Mongolian National University of Medical Sciences, where discussions were held regarding potential future collaboration.
A particular highlight of this year’s training was the introduction and application of the self-gripping mesh, which enables automatic fixation to the abdominal wall without additional suturing.
5. Surgical Procedures Performed
Darkhan-Uul Provincial General Hospital
• Total surgeries performed: 21
• 11 open surgeries
• 10 laparoscopic abdominal surgeries
• 3 pediatric hernia surgeries
Second State Central Hospital
• Total surgeries performed: 21
• 16 open surgeries
• 5 laparoscopic abdominal surgeries
6. Conclusion
The program successfully strengthened the clinical experience and theoretical knowledge of Mongolian surgeons and healthcare professionals in advanced hernia treatment methods. The ongoing cooperation with the International Hernia Foundation continues to play a vital role in surgical capacity building, international partnership development, and the adoption of modern hernia repair technologies in Mongolia.








Report prepared by:
Z. Sonor — Colorectal Surgeon, General Surgery Department, Second State Central Hospital
Reviewed by:
Ts. Narmandakh — Honored Doctor of Mongolia, Consultant Surgeon, Second State Central Hospital
International Team to Nyandarua, Kenya. 16-20 Nov 2025
International Team to Nyandarua, Kenya. 16-20 Nov 2025
HERNIA INTERNATIONAL MISSION TO KARIUKI MEMORIAL COUNTY REFERRAL HOSPITAL, NYANDARUA COUNTY, KENYA.
NOVEMBER 16-20, 2025. STATUS: COMPLETED
Coordinator: Dr. Gachara Boniface (Kenya), coordinator Samuel Wainaina (Kenya), Medical
Superintended Beatrice Mugure (Kenya), Team leader Thorbjorn Sommer (Denmark).
The International Team: Steve Lindley, (UK), Heidi Miller (USA), Thorbjorn Sommer (Denmark), Soeren Pedersen (Denmark), Clara Scheffmann Gosvig (Denmark), Lene Scheffmann Gosvig (Denmark).
Total: 6 volunteers

TECHNICAL REPORT
DATES AND LOGISTICS DEPLOYED:
Campaign conducted November 16-20, 2025.
ADULT PATIENTS: Hernias (inguinal, umbilical, ventral, inguinoscrotal), lipomas, hydroceles.
PEDIATRIC PATIENTS: Hydroceles, umbilical hernias, inguinal hernia.
CONSULTATION AND SURGERY PERFORMED:
Patients seen in consultation: 104
Number of cases performed: 93
Complications: one week after termination of the camps no complications has been seen according to Dr. Jairus Ochieng.
For statistics please see Power Point from Dr. Gachara Boniface previously posted on this website.
CAMPAIGN SUMMARY
JM Kariuki Memorial County Referral Hospital
The Hospital is a major referral center for about 700.000 people living in Nyandarua County. It is located 3,5 hours’ drive north of Nairobi. The Hospital is under constant
development with new departments and development of various health projects. The hospital consists of different departments: Surgical department, emergency department,
Intensive care (4 beds), medical care, vaccinations center, facilities for child-mother care,
maternity, laboratory and testing etc, CT and Ultrasound scanning facilities.
Concerning the surgical department there were two operation theatres, with two tables each of which three was used for the current Hernia mission, while the other was used for caesarean sections. Other types of surgery (like ortopedics) were directed to other hospitals during the Hernia mission. As such it was possible to perform 3-4
operations simultaneously, which we found very efficient, making it possible to discuss difficult cases across the room.
The Kenyan side of the team had done a very efficient job and they were prepared for the mission. During the mission we also had a visit from a TV Team together with the Governor who took his time to visit the hospital accompanied with the bishop and CEO´s of the region and hospitals The recording from the visit went on live TV during the mission. This created further knowledge among the community about the possibility to get surgery for hernias.
The video can be viewed here: https://www.facebook.com/reel/1297884622024993. We had a lot of good experineces from the mission last year, which made it very easy to continue our cooperation in developing fast track surgery.
The operating theatres were well equipped with air conditioning, allowing for a comfortable work
environment. Power cuts were rare and did not affect our work.
The hospital was equipped with three diathermy machines, and we monitors for patient surveillance in the recovery room/ICU donated by Private Hospital Molholm in Denmark. The Team members brought each what was possible to collect of up-to-date equipment (gowns, sutures, scalpels, drapes, dressings, meshes, local analgesics etc.). We had a terrific cooperation with the local anesthesiologists George, Esau and Daniel and Kariuki
making it possible to do surgery under general or spinal anesthesia. Local anesthesia was used in selected cases.
The General Surgeon at the Hospital Jairos Ochieng is a very hard working and skilled general surgeon, and we had a very inspiring and joyful time together discussing treatment options in individual patients, indications for surgery and of course also technical aspects of Hernia surgery.
We did ward rounds every morning to see the postoperative patients from the previous days before discharging them. In between surgery we saw patients who requested screening for a variety of surgical/non -surgical diseases, and patients coming for check-up after surgery.
The patients were seen dressed in gowns ready for surgery in a room in front of the theatre where they were marked by the operating surgeon before the operation They were informed about surgery, written information about the surgery, operative procedure, risks etc. and consent of the operation was ensured. Cleaning between the shifts were swift, making it possible to do fast track surgery Patients were schedules to stay in the ward to the following day, where they were seen before
discharge.
THE TEAM
The team consisted of three surgeons: Steve Lindley (UK), Heidi Miller (USA) and Thorbjorn Sommer (Team leader Denmark). Anesthesiologist Søren Pedersen, (Denmark) Anesthetic Nurse Lene Scheffmann Gosvig (Denmark) and Clara Scheffmann Gosvig (assistant., Denmark) assisted with the procedures together with the local staff. Two months before departure we had 2 virtual Zoom meetings, with participation of our Kenyan colleagues, where we were introduced to each other, discussed the mission, the need of equipment to the Hospital.
TRAVEL/VISA/PERMITS
Travel to Kenya is easy since there are a lot of departures to Nairobi. eVISA must be obtained (online) before departure. Samuel did a terrific job securing Temporary Surgical License to the surgeons operating before arrival. We had a challenge to get out equiopment through customs, since there a new rules concerning donations in Kenya: Exemption for tax on donations should be acquired before arrival. Our Kenyan
staff had to pay a tax of 11.115 Shilling (86 USD) in Tax before we were allowed to take our
donated stuff with us to the Hospital.
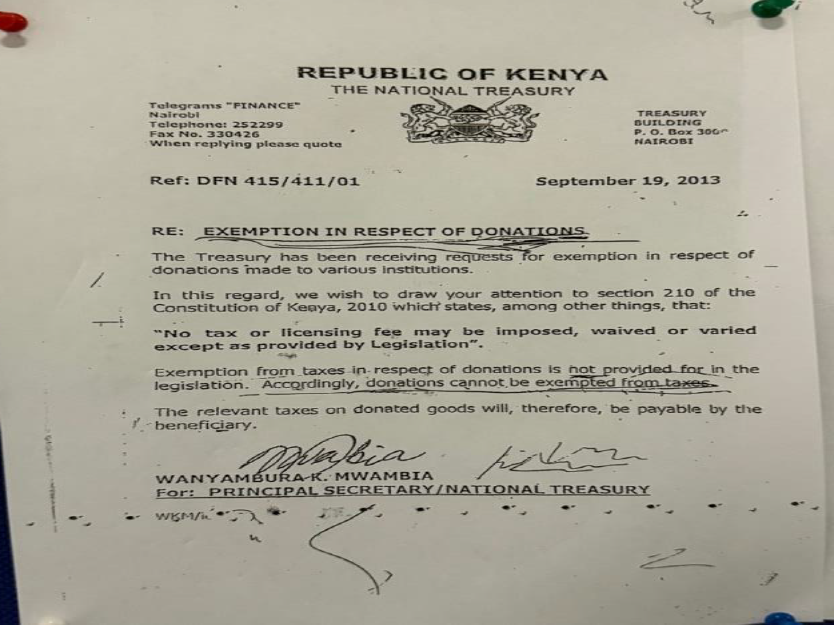
SCHEDULE
Our routine included Breakfast at 7.30 AM before starting surgery at 8-8.30 AM. We had a lunch break at 2 PM, and finished the last surgery between 4 and 8 PM, depending on the
number of cases scheduled. Thursday night a party was arranged at the Hotel together with all the staff, local organization and everybody involved in the Hernia Camp with tasty food, a lot of good talks and the team members
were granted with gifts, which we all are very thankful for.
LOCAL STAFF
The local staff had done a significant job in recruiting patients using various channels such as posters, newspapers and radio advertising, ensuring we had a sufficient amount of patients. Especially after the news about Hernia surgery upon the governers visit secured a lot of patients, some coming from afar (+500 km away).
Arriving at the Hospital all patients were carefully registered and prepared before being seen by a surgeon prior to surgery, with evaluation and marking of the hernia. It was an important and primary focus of all staff to ensure patient safety from the first step.
Doctor Aisha and nurse Lucy were phenomenal to arrange everything logistically, kept the files in place, knew were the next patient was and where the previous should go.
The Medical Superintended Beatrice Mugure did a terrific job with competent overview of the organization. Extra personnel had been called in, so we were well equipped with competent staff from anesthesia, surgical and ward
assistance, making it possible to upscale the number of procedures. Safe check in was performed before initiating surgery. Working together with the local staff was a very positive experience for all of us, sharing expertise, skills, technical tips and ways to go forward in the care of
hernia patients as well as keeping a good spirit, lots of laughs, hugs and good humour.
EQUIPMENT
The Hospital was well equipped, and the Team brought what was possible for each member to collect from their home Hospitals of new equipment. Private Hospital Moelholm donated monitors for further use in the recovery/ICU rooms.
ANESTHESIA
The Theatres were equipped with ventilators and at each operative table, there was monitor with a pulse oximeter and a blood pressure cuff, and ECG. Anesthesia was obtained using Ketamine, Halothane, Propofol and Desflurane, spinal or local anesthesia. The majority of patients received local blockage with Marcaine as post operative pain treatment together with Paracetamol and Ibuprofene. Having an anethetic team with us working together with the local anesthetisist was very valuable, and different ways to do anestesia in safe ways were discussed and developed.
ASEPSIS AND SURGICAL MATERIAL
All patients had washed before arrival for surgery. At the hospital they were washed with
appropriate antiseptics, hair was removed, the site of operation was preoperatively marked on the skin and local anesthesia was applied. All patients received a single dose of Ceftriaxone as SSI profylaxis. The local staff practiced aseptic procedures making it easy to secure clean procedures. Sufficient surgical material boxes were available.
ACCESSIBILITY FOR THE POPULATION
Before our arrival, the Hospital had conducted an information campaign with information about the possibility of hernia surgery. The patients paid a small fee, what they could afford, some came a
long way to be operated (many hours of transportation).
ACCOMODATION IN NUANDARUA
Again we stayed at the nice 818 Hotel situated 1 km from the Hospital, making a short morning walk possible. The Hotel had a very nice staff, nice spacious rooms with aircon, clean bathrooms, a nice restaurant with a variety of local and international meals. However, the best was a Tusker Beer after long working hours.
CONCLUSION
Strengths:
The Hospital is not too far away from Nairobi Airport, reducing time for transportation to a
minimum. Transportation is swift and well organized. Patients came from far away, and the standard at the facility made it easy to do high-volume Surgery with good quality in every aspect. Accommodation is nearby so no time is wasted on transportation.
The staff is very well educated and a tremendous help in assisting us with everything. They have the capacity to raise awareness of Hernia surgery, planning a comprehensive surgical camp and secure patient safety in a high-volume setting. It is highly recommended to further develop Hernia Camps in Nyandarua, since all capacities for further hernia surgery is present. There is also a wish to do laparoscopic hernia surgery in the future, and if it would be possible to provide laparoscopic equipment it would definitely be the place to do it.
Things we might do differently:
Among a variety of strategies we worked on: preparation for each case in the theatre making sure all equipment was available, which kind of anesthesia was intended and what kind of hernia was to be repaired in which patient – should be known before bringing the patient to the theatre.
- Keeping things in order on the tables, ensuring a low risk of substitution of drugs and
instruments. - having a pecific contact person in the morning when doing the reounds to identify patients from the previous day, ensuring everybody was seen would be a good value as well, shortening time to the rounds making more time at the theatre possible.
- engagement of local media, especially TV shortly before the mission would be of great value concerning patient recruitment. Videos taken this year could be used on social media referring to the possibility of surgery in Nyandarua.
In conclusion we again highly recommend Hernia Missions conducted on an annual basis in Nyandarua from Hernia International.
On behalf of the Team 2025
Yours sincerely,
Thorbjorn Sommer
Head of International Team to Nyandarua
November 2025


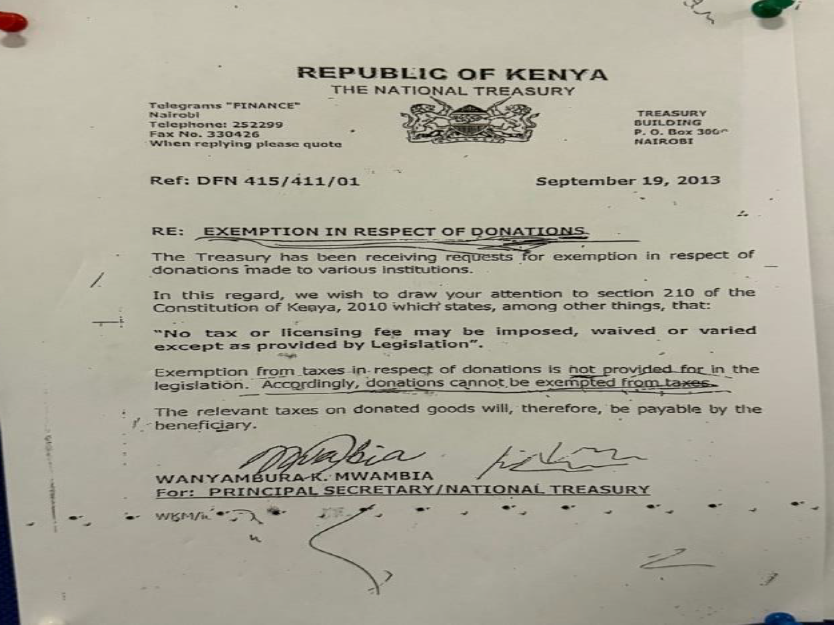












International Team in Dangbo, Benin. Nov 2025
Team members:
Petr Bystricky (Surgeon, Czechia)
Michael Brownstein (Anaesthetist, Australia)
LiLin Hong (Anaesthetist, Australia)
Heidi Miller (Surgeon, USA)
Cea-Cea Moller (Surgeon, Australia)
Dominique Robert (Surgeon, Australia/France)
Richard Turner (Surgeon, Australia)

I had previously undertaken Hernia International missions to the Auberge de l’Amour Redempteur, Dangbo in 2017 and 2018. Returning this year, even just arriving at Cotonou Airport, it was evident that Benin had experienced a quantum leap forward in terms of its economy and the reforms that were taking place across all sectors of society. The first inkling of this, some months before the mission started, was the requirement to provide detailed, certified documentation regarding team members’ citizenship, medical and speciality qualifications, and credentialing in their respective home countries. Although this is a routine requirement for most missions, the fact that it was not such an issue pre-COVID suggests that the government is keen to rein in unscrupulous operators. Fair enough.
Once the above documentation was approved by the Ordre National des Médecins du Bénin, some weeks after we had submitted it to our host (Dr Sr Opportune Tosse), a letter was produced detailing each team member’s role and responsibilities. This in turn had to be sighted and approved by the Ministry of Health before we could commence our mission. Due to procedural delays, this final official sign-off could not occur until the morning of our first operating day. We were more or less assured that this would be a rubber-stamp process, so we spent the previous day (a Sunday) assessing the 50 or so patients that Sr Opportune had previously triaged. By the end of the day, we had scheduled approximately 45 cases for the coming week. These were predominantly large inguinal/inguinoscrotal hernias in adult males, a few hydroceles, and occasional skin lesions – including one highly disfiguring keloid in a young man, which was eminently resectable and had the assurance of adjuvant steroid injection.
I had a sinking feeling that something was seriously wrong when Sr Opportune came to my accommodation at 0730h on Monday morning. A surprise curveball had been thrown overnight. The Ministry would not approve our mission unless it was sponsored by a local specialist. Despite her medical degree, Sr Opportune did not qualify, as she was not a surgeon, nor did she have any immediate contacts to call upon at the last minute. If we had put knife to skin, we would have risked imprisonment!
The November 2025 HI mission to Dangbo was therefore over before it started. The nuns continued to kindly feed and entertain us for a couple more days before we dispersed. Because the Ministry would normally require three months to vet a potential sponsor Sr Opportune will need to cancel two other specialist missions in the coming months. Like us, I daresay those people have already booked airfares and leave from their usual work.
Reflecting on this sorry episode, I do not feel that official corruption played a part. No amount of ‘payment from the heart’ could have allowed us to proceed. Our mission, like many others, fell victim to the justified raising of standards in health care in low-middle income countries. The real grievance relates to the poor communication from some bureaucrat in the Ministry of Health – almost as an afterthought – that we required a local sponsor they knew we would not be able to get in the timeframe. It felt awfully like someone wanting to exercise their power and superiority over a group of foreign do-gooders. Beyond this, Sr Opportune indicated that there were new accreditation standards that would need to be achieved for future surgical missions, the main ones being a second operating room (at present, there are two tables in one room) and a dedicated recovery area. Both of these require a major upgrade of existing infrastructure that will be extremely difficult to achieve in the foreseeable future without a major injection of funding. Failing this, operating capacity would be halved. On a more positive note, very little equipment, instrumentation, or medications need be brought by other hernia missions for the next year or so, thanks to the ample supplies brought by recent Spanish missions.
Would our team ever want to return to Dangbo? I certainly would, in a heartbeat. The dedicated personnel are a pleasure to work with, and the patients are extremely grateful for our services. No local specialist in the region has the capacity to do this work, unremunerated, for people who cannot afford their services. For future missions, the following would conditions need to be met.
- Notification of intention to conduct mission 12 months in advance.
- Nomination of anaesthetic and surgical team members as soon as possible after this, and submission of necessary paperwork to hosting hospital: passport details, medical and specialist diplomas, and evidence of current registration to practice in home country. At least two team members should have a working knowledge of French.
- Approval of the above documents by the Ordre National des Médecins du Bénin.
- Letter of support/invitation from suitable local specialist no later than 3 months from the mission commencement date.
- Ministry of Health approval of the team members’ accreditation and the sponsoring specialist, well in advance of the mission commencement date.
Team members are also advised to book refundable airfares!
Prof. Richard Turner
Chef de Mission, Dangbo 2025
28 November 2025
Danish-UK-USA team to Nyandarua, Kenya. Nov 2025