
MAKURDI CAMPAIGN, NIGERIA. NOVEMBER 2025
- INTRODUCTION
On this occasion we organized in collaboration with Hernia International a campaign at the Bishop Murray Medical Center in Makurdi, Nigeria, where at least three previous campaigns have already been carried out, the most recent one in May 2025.
The core group initially consisted of four members from a campaign carried out the previous year in Sierra Leone. Thanks to a call made by Dr. Butrón Vila to volunteers from the Cirujanos en Acción Foundation, the group was quickly completed, ultimately forming a team of 14 people.
- TECHNICAL REPORT
2.1 DATES AND LOGISTICS
The campaign was organized for the week of November 14 to 23, 2025.
We assembled a team of 14 people with the idea of working on three operating tables, based on the information provided by members of the previous campaign: one table for general surgery (hernias) with spinal anesthesia, one table for thyroid surgery with general anesthesia, and another table for pediatric surgery with general anesthesia.
We purchased the airline tickets through Ángelis, an agent from Halcón Viajes who usually manages this process for the Foundation’s campaigns. Six people departed from Madrid, five from Barcelona, and two from Vienna. We all met in London and from there took the flight to Abuja. Once in Abuja, we met Salifuo, a team member who traveled independently from Niger. Following the advice of the previous team, we hired a bus service from Abuja to Makurdi for €85 per person (round trip) through Austin Ella, our local contact in Nigeria for the campaign.
As with the previous campaign, the main problem was obtaining visas. Although on this occasion the electronic visa was available at a cost of €256 for a tourist visa, the Nigerian Immigration Service operates erratically. We encountered three scenarios: some obtained the visa without major difficulty in less than 24 hours; others were initially denied and had to reapply (and pay again) to obtain it; and a third group received no response at all (neither approval nor denial). Despite having initiated the process in September (more than two months before the travel date) and sending multiple emails, we were unable to determine the cause of the problem. The Madrid embassy disclaims responsibility for the electronic visa and refers applicants to the Nigerian Immigration Services in Abuja.
On the day of departure, two team members still did not have their visas, which forced us to go to the Madrid embassy on the same day as the flight to seek a solution. Thanks to Jasper Suleiman (an embassy employee) and the ambassador’s secretary, we obtained the visas barely three hours before departure.

For all these reasons, we recommend that teams for future campaigns carefully complete the visa application with the exact passport details and thoroughly review the emails received, including spam folders, ensuring that the acceptance or denial document is received. The process should be started with sufficient time to address potential issues, but not earlier than three months in advance, which is the validity period of the visa.
We also discussed the visa difficulties with Austin Ella, who assured us that for future campaigns he will try to have a contact within the Immigration Services to expedite the process.
Furthermore, we agreed with him that, for future campaigns and in order to avoid legal issues, team members should be registered with the Medical Council, the body responsible for regulating physicians and ensuring good medical practice in Nigeria. This is a procedure that must be carried out by local staff, and in the last two campaigns no such registration had been completed, leaving all responsibility with Dr. Thaddeus, the physician at Bishop Murray Medical Center.
On the day of our arrival at the airport, Dr. Thaddeus met us at the baggage claim area and assisted us with customs clearance. This is always a critical step since, although on this occasion we carried anesthetic medication with an export report from the Spanish Agency of Medicines, luggage is often inspected in an attempt to demand money.
This time we encountered difficulties due to material that was close to expiration or already expired (upon entry they require expiration dates of more than six months, which is reasonable). Thanks to Dr. Thaddeus’s mediation and after a payment of approximately €120, we were able to bring everything in.
SURGICAL PROCEDURES (Annex 1)
Two weeks after our return, we contacted Dr. Thaddeus, who informed us that he had not received any complicated patients.
- CAMPAIGN REPORT
3.1. LOCATION
Nigeria is a West African country bordered by Niger to the north, Chad to the northeast, Cameroon to the east, and Benin to the west. Its southern coast lies on the Gulf of Guinea in the Atlantic Ocean. The federation comprises thirty-six states and the Federal Capital Territory, where the capital, Abuja, is located.
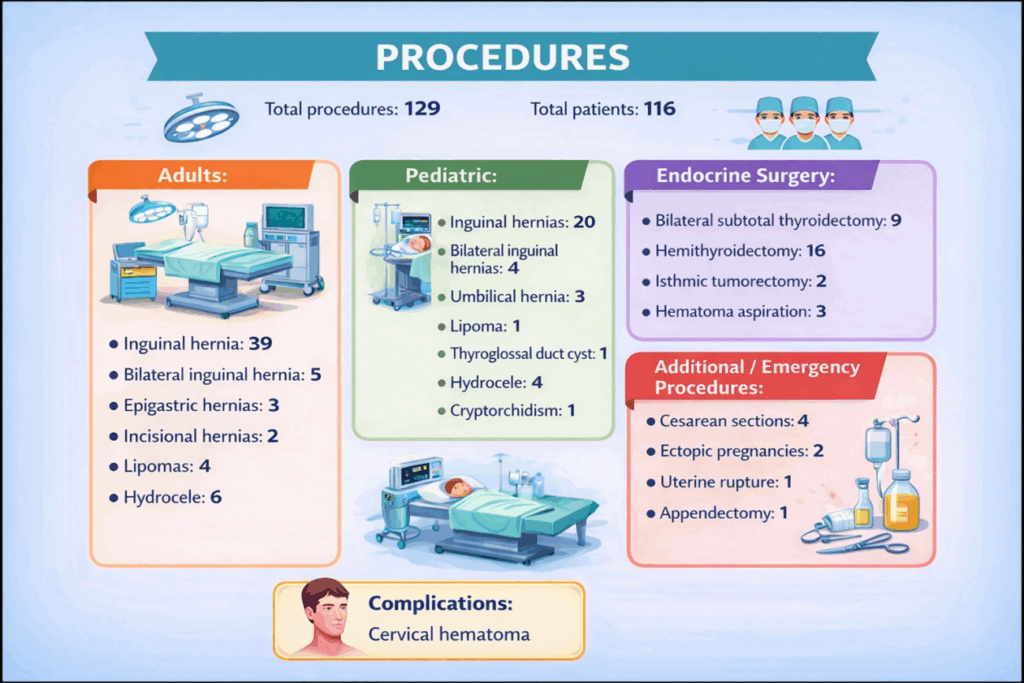
The Bishop Murray Medical Center is a hospital located in Makurdi, about 300 km southeast of the capital (almost six hours by bus). It is a healthcare center belonging to the Catholic Diocese of Makurdi. It is a simple but well-equipped center with radiology services, operating rooms, laboratory, sterilization, etc. It has several inpatient wards separated by gender and some private rooms without nursing services.
We stayed in a diocesan residence free of charge, in single rooms with air conditioning and private bathrooms—simple but adequate. The hospital is about a 15-minute drive from the residence.
3.2. TEAM
Coordinator: Sebastián Fernández Arias
Nurses: Estela Sala Carbellido, Pilar García Diez
Anesthesiologists: Maribel Real Navacerrada, Paula Alejandra Morales, Antonio Hinojosa Jiménez
Endocrine Surgeon: Enric Caubet
General Surgeons: Lucia Catot Alemany, Elisabet Julia Verdaguer, Elisabeth Redondo Villahoz
Pediatric Surgeon: Valeria Solari
Pediatrician: Johanna Würzl
Support Staff: Gloria Hospedales i Catot, Salifou Hankouraou
3.3. LOCAL STAFF
Our contact in Nigeria was Dr. Austin Ella, who acted as our liaison with the Diocese to coordinate all pre-departure arrangements. The Medical Director of Bishop Murray Medical Center was Father Peter Paleve, who looked after us throughout the campaign.
In Makurdi we were accompanied by Dr. Thaddeus, a general practitioner with surgical knowledge, with whom we addressed issues related to equipment, patients, etc. He was also responsible for patient selection and for organizing the daily surgical schedules. Although there were enough patients to fill the daily workload, it is advisable to agree in advance on the expected activity, since in our case approximately 50 thyroid surgeries were scheduled over six days, which proved unfeasible, and on the last day there were no pediatric patients.
During the working week we collaborated with Jacob, Nicholas, Timothy, and Joshep, who were responsible for patient transport and worked efficiently and tirelessly.
Similarly, Bridget, Charity, and Josephine were in charge of sterilization to ensure all material was ready, and Benedicta assisted our anesthesia team.
3.4. EQUIPMENT
The Bishop Murray Medical Center is well equipped and has the necessary resources to carry out a campaign involving procedures under spinal and general anesthesia.
The surgical area consists of a large room that allows the installation of several operating tables simultaneously, separated by screens. It has air conditioning and an electrical supply with generator support, although surgical lighting is limited, making the use of headlamps necessary for some procedures.
The hospital has two electrosurgical generators, one of which required repair during the campaign. The team provided two additional generators (one from the Foundation and one from Dr. Catot), which allowed simultaneous work on four tables.
It also has a Dräger ventilator with a Philips monitor, which made it possible to perform procedures under general anesthesia (additional anesthesia-related information is provided below).
The Radiology Service has an older ultrasound machine, which Dr. Caubet used to assess all patients scheduled for goiter surgery.
The team provided pulse oximeters and a portable blood pressure monitor, which proved useful during the campaign. The hospital did not have these devices, and they were left there at the end of the campaign.
3.5. ANESTHESIA
3.5.1. Operating Area and Recovery
Within the surgical area, the center has a Dräger Atlan 300 anesthesia machine with a Dräger Vista 120 monitor, including gas monitoring and capnography, as well as two basic monitors (pulse oximetry and non-invasive blood pressure).
There is no structured post-anesthesia care unit, so an area adjacent to the operating room was designated for postoperative monitoring, especially for patients undergoing thyroid surgery. In this context, the finger pulse oximeters and portable blood pressure monitor provided by the team were extremely useful.
3.5.2. Anesthetic Techniques
During the campaign, general anesthesia, spinal anesthesia, and sedation techniques were used, adapted to the pathology and available resources.
Pediatric anesthesia was performed using inhalational anesthesia with a laryngeal mask under spontaneous ventilation, combined with regional blocks, using a sevoflurane vaporizer and a Mapleson-type ventilation system provided by the team, with oxygen supplied via cylinders. The high gas consumption required local purchase of sevoflurane at a high cost.

In thyroid surgery, the Dräger Atlan 300 ventilator allowed safe general anesthesia, although without the availability of medical air. Anesthetic maintenance with propofol was possible thanks to the intravenous infusion pump provided by the team. Given the nature of the pathology, it is strongly recommended to bring a videolaryngoscope, which allowed resolution of two difficult airway cases using a King Vision device and a Frova-type guide.
One episode of severe bronchospasm was recorded, which responded to standard treatment. Postoperative cervical hematomas were drained under sedation. Ketamine proved particularly useful in this setting.
For adult abdominal wall surgery, spinal anesthesia was used without significant incidents. At one operating table, monitoring equipment provided by the team was required.
Due to a strike at the other hospital in the city, unforeseen emergency cases were treated, including cesarean sections, ectopic pregnancies, a uterine rupture, and a perforated appendicitis. Cesarean sections and ectopic pregnancies were performed under spinal anesthesia; more severe cases required general anesthesia with orotracheal intubation. The patient with uterine rupture required advanced cardiopulmonary resuscitation, central venous access, and whole blood transfusion, evolving favorably despite the absence of an ICU at the center.
This experience highlights the importance of bringing emergency equipment and medication, which on this occasion could be partially obtained from previous campaigns.
3.5.3. Materials
During the campaign, local resources and materials provided by the Foundation and by team members were used.
A need was identified for future campaigns to have a larger supply of tranexamic acid, antihypertensive drugs (especially labetalol), opioids such as fentanyl—very difficult to obtain locally—as well as a greater number of three-way stopcocks and extension lines.
The usefulness of materials from previous campaigns was confirmed. At the end of the mission, medical supplies and medications were left under proper custody with a detailed inventory.
3.5.4. Training Impact and Knowledge Transfer
Given the absence of formally trained anesthesiologists, practical training was provided to Benedicta, the nurse responsible for anesthesia, in airway management techniques (including videolaryngoscope-guided intubation with an Airtraq-type device), general anesthesia, and pediatric anesthesia. Practical teaching was also provided to nursing staff and nursing students to assist in pediatric surgical procedures.
3.6. ASEPSIS AND SURGICAL MATERIAL
The sterilization room adjacent to the operating theater has two or three pressure-cooker-type autoclaves in which all material was sterilized. We brought surgical material from the Foundation distributed in six boxes (two for thyroid surgery and four for hernias), which were sterilized in small cloths. Before starting the campaign, all material was labeled. Dr. Solari also brought pediatric surgical instruments.
The main limitation encountered was with surgical gowns, as we did not bring enough for the entire campaign (they take up a lot of space and are not easy to obtain). As a result, we had to use cloth gowns from the hospital and re-sterilize some of the gowns we had brought.


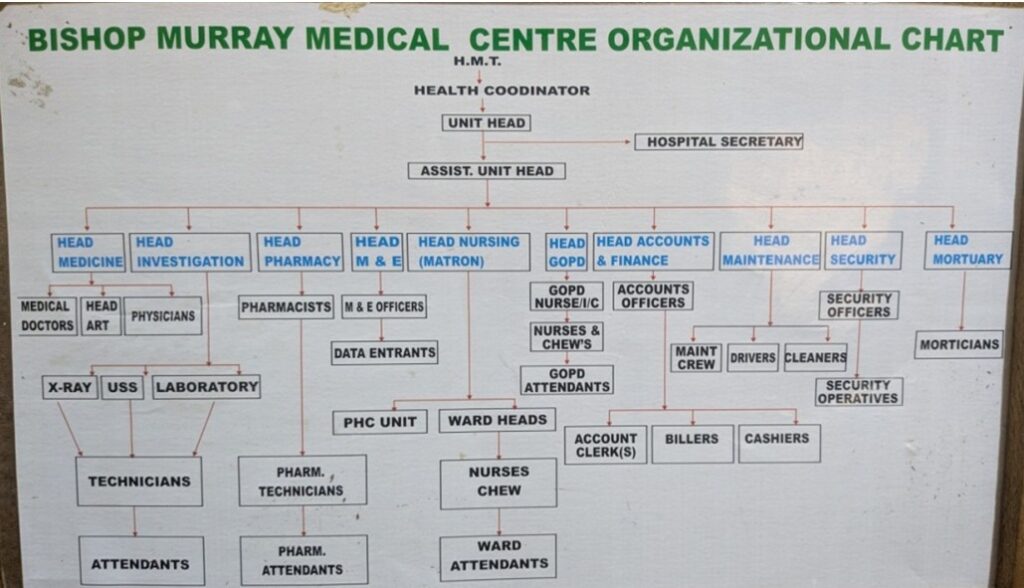
We established a basic set for a standard hernia procedure, which was used for most of the interventions, consisting of:
- Sterile gloves for the team and gowns
- Antibiotic
- Antiseptic
- Scalpel blade
- Syringe for local anesthesia
- Large sterile drape (150 x 180 cm) for the patient
- Small sterile drape (50 x 50 cm) for the table
- Mesh
- Electrosurgical unit
- Sutures (PDS 2/0 x 2 for the mesh and Monocryl 3/0 triangular needle for the skin)
3.7 DAILY LIFE IN MAKURDI
On the day of our arrival at Abuja airport, Dr. Thaddeus met us at the baggage claim area and assisted us with customs. Dr. Austin Ella was waiting for us in the parking area. We traveled by bus to Makurdi without any incidents.

On Saturday, the day of our arrival, we were welcomed at Bishop Murray Hospital with a welcoming ceremony where we met all the hospital staff. That same day we took the opportunity to organize and store all the material.
On Sunday, we were welcomed again at the diocesan mass early in the morning, and from there we went to the hospital to begin the surgeries.During our stay in Makurdi, we stayed at the diocesan residence about 15 minutes by car from the hospital. We usually met in the dining room around 6:45–7:00 a.m. for breakfast (coffee with scrambled eggs or pancakes), and at 7:30 a.m. we were picked up to go to the hospital to begin the surgeries.


The typical day consisted of reviewing patients operated on the previous day and assessing those scheduled for surgery that day. The surgical day usually started around 9:00 a.m. and ended around 8:00 p.m. We stopped for lunch between 1:00 and 2:00 p.m., although most of the time we ate in groups depending on the surgical schedule. At the end of the day, we were picked up again from the hospital and finished the day with dinner together in the residence dining room.
On the last working day, during lunchtime, a farewell ceremony was held and we were presented with honorary garments as gifts.


Outside the hospital there were not many leisure options, or at least none were recommended to us. On the last day, while part of the group organized the remaining material and packed all the equipment we were bringing back (a list of materials left behind is included in Annex 2), another part visited a local market and made some purchases (mainly fabrics).

We left Makurdi the day before our return flight and stayed the last night in Abuja, in a diocesan residence similar to the one in Makurdi and very close to the airport (about 20 minutes away). As we had incurred some unforeseen expenses during the campaign (some medications and airport “fees”), it was agreed that the hospital would cover the accommodation in Abuja, so there was no cost to us. We had dinner at the residence and left for the airport at 6:00 a.m. the following day.
The return trip proceeded without incident, and in London we said our goodbyes and continued on to our respective destinations.
3.8. TOTAL COST OF THE CAMPAIGN
Estimated total cost: €17,831.40 / 13 people* = €1,371.65 per person.
*Estimated expenses related to the 13 team members from Spain and Austria.
Flights: (Vienna €972.35, Barcelona €1,033.73, Madrid €1,056.15). Total: €12,416.52
Insurance: €48.50 (price from Spain**) ≈ €630.50
**Ten people purchased insurance through an agency; one traveling from Spain and the two from Vienna purchased it independently. It is estimated that the cost was the same for all 13 people for calculation purposes.
Visas: €256 x 13 = €3,328
Bus transport between Abuja and Makurdi: €1,106.38
Additional expenses: approximately €350 (airport “fee” for materials €120 + purchase of Sevoflurane)
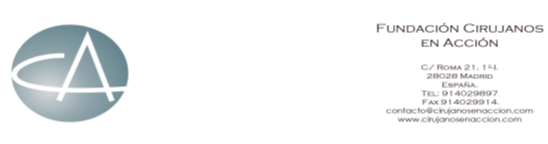
ANNEX 1
SURGICAL PROCEDURES
Total procedures: 129
Total patients: 116
Adults:
- Inguinal hernia: 39
- Bilateral inguinal hernia: 5
- Epigastric hernias: 3
- Incisional hernias: 2
- Lipomas: 4
- Hydrocele: 6
Pediatric:
- Inguinal hernias: 20
- Bilateral inguinal hernias: 4
- Umbilical hernia: 3
- Lipoma: 1
- Thyroglossal duct cyst: 1
- Hydrocele: 4
- Cryptorchidism: 1
Endocrine Surgery:
- Bilateral subtotal thyroidectomy: 9
- Hemithyroidectomy: 16
- Isthmic tumorectomy: 2
- Hematoma aspiration: 3
Additional:
- Cesarean sections: 4
- Ectopic pregnancies: 2
- Uterine rupture: 1
- Appendectomy: 1
Complications:
- Post-thyroidectomy hematomas: 3
ANNEX 2
INVENTORY OF MATERIAL LEFT AT THE HOSPITAL
- Gloves size 7.5: 50 units
- Disposable sterile forceps (14.5 cm): 8 units
- Dressings: Various
- Mepilex (silicone dressings 10 x 18 cm): 20 units
- Surgical drapes:
- 100 x 80 cm: 15 units
- 150 x 180 cm: 10 units
- Fenestrated (75 x 90 cm): 8 units
- Argenpal (skin stick): 5 containers
- Electrosurgical pencil tips: 20 units
- Fluid controller (flow regulator): 12 units
- Peripheral IV dressings: 300 units
- Mefix 20 cm x 10 m: 3 units
- Scalpel blades: No. 11 (200 units), No. 15 (50 units), No. 23 (250 units)