MEMORY OF THE MISSION OF “CIRUJANOS EN ACCIÓN” AND “HERNIA INTERNATIONAL” IN FREETOWN (SIERRA LEONA) ON 15-23 JUNE 2019
(Police Hospital and Connaught Hospital)
This has been the first mission that “Cirujanos en acción” (CA) and “Hernia International” (HI) have carried out in Sierra Leona. The initial place for this mission was the Makeni district in the inner country, a zone needing badly surgical help in hernia pathology according to the request of contact with HI at the end of 2018, but due to logistic problems it took place finally in the capital of the country, Freetown, and simultaneously in 2 public hospitals, the “Police Hospital” (PH) and the “Connaught Hospital” (CH).

The “Cirujanos en Acción” team was formed by 10 persons according to the needs of the initial campaign. Four general surgeons: Cesar Ramirez (Málaga), Teresa Butrón (Madrid), Hermelinda Pardellas (Vigo) and Guadalupe Moreno (Ibiza); a paediatric surgeon, José M. Morán (Badajoz), three anaesthetists, Salvatore Catania (Huesca), Beatriz Fort (Barcelona), and Sandra Casares (Ibiza); and, to complete the team, two nurses, Francisco Gomez (Malaga) and Silvestra Barrena (Madrid).

The previous coordination, after the last moment discarding of Makeni’s destiny, has been very troublesome; in order to organize everything we had the great help of Dr. Biku Ghosh, an Indian surgeon, working in the UK for many years, who usually volunteers with the “Saving Lives” ONG and who had just finished a mission in Freetown. The key contact persons in Sierra Leona have been at PH Dr. Paul Fillie (responsible surgeon) and Dr. Mohammed Jalloh (director in charge), and in the CH Dr. Samba Jalloh (a young “practitioner” of Freetown very much implied in coordination work of humanitarian missions) and Dr. James Boima (surgery chief in that centre and high prestige surgeon and national consideration plus absolute reference, of Sierra Leone).

The starting point of each of the team members were their cities of origin, and we all got together at the Paris airport to begin the flight to Freetown. We arrived to our destination on Saturday 15th late in the evening, and we were received at the airport by Dr. Paul Fillie. More than 20 pieces were booked with more than 350 Kg of material, and in this occasion I want to underline the Air Europa collaboration as they allowed us to travel with excess luggage without additional cost. The Freetown airport (Lungi International) is very far from the city, in a gulf that makes it necessary to take a “ferry” for about 35-40 minutes to arrive, as otherwise there are almost 4 hours by car; this forces us to arrange the times of arrival and of leaving the country in function of the times of the ferry. On reaching the city and disembarking we got a warm welcome by the PH staff, and besides that we had a bus of the Sierra Leone Police for our displacements in the city.

Our stage was arranged in The Jam Lodge, a fairly central hotel which had been recommended by Dr. Ghosh and which we had booked by “Booking.com” previously. It is a decent hotel, with hot water, a good breakfast and in which the Wifi works not good; the price or the room is about 50 dollars a day for single or double room. We daily gathered at 7 a.m. in the morning to plan the day, and at 8 a.m. the bus came to take us. We had a great help in Suleiman Conteh, a young student of political science, who has experience in helping humanitarian missions and who every day sent us food and drink in the two hospitals; the price of food and drink has been about 3 dollars for person a day, but as in both hospitals we paid for food for the whole staff that worked with us the increment was important (we have paid on an average 150 dollars a day for food). The local money is the “lion”, but in fact everybody works with American dollars and this is what we used. On Friday 21st June night, after the last word in the operation theatre, Dr. Mohammed Jalloh was kind enough to invite our whole mission staff and operation theatre PH staff to a common dinner which was very much appreciated and valued.

The process of gathering and selecting patients by Dr. Fillie in PH has been really good, so that there were more than 250 patients ready to be examined, the majority with a severe hernia pathology, which we evaluated on Sunday 16th June along morning and evening; in CH there were hardly 30-35 patients selected, some of them with small hernias, all selected by Dr. Boima. In PH there was only one respirator and two operation theaters; in CH we also had one respirator and two operation theaters (both with respirator, but one of them only for children) and this was the first problem we have met as the flow of PH patients to be operated upon in CH was not the desired one, and the administrative facilities have not been good either. Finally, in CH we were given on the last days a third operation theater so that we could fulfill the expectations we had come with. In the PH there was no facility for sterilization of the material so that everything had to be sent to the CH, and this has always been a problem from the logistic viewpoint. Even so, given that we have some boxes of surgical material of our own for children and adults that we had taken from Spain we have been able to help in this. In the PH only an electric scalpel was working and it was of poor quality, that is why we have been able to operate effectively in only one room; in CH they have two electrical scalpels, but only one was working properly, so that it has been fundamental that we had brought from Spain an electrical scalpel provided by Teleflex. CH is a large hospital with more than 200 beds, while in PH there are no more than 30 beds, and this, given the bad coordination between both centers has also brought logistic problems shifting from one centre to another, and this has created internal tensions, sometime unpleasant. From our part, and given that children could be operated upon only in CH, we have decided to divide the team in 2 working groups, one with an anaesthetist, a lady nurse and two general surgeons for the PH and another with two anaesthetists (one of them specifically for children), two general surgeons for the PH and another with two anaesthetists (one of them specifically for children), two general surgeons, one paediatric surgeon and a male nurse for the CH. I can say that it has not been a good experience, and I do not recommend that in future campaigns we work in two hospitals at the same time, and divide the team members even more in countries where we cannot communicate by phone between us because there is neither an accessible phone neither an accessible phone line nor wifi for “whatsapp” communication between hospitals.

On Monday 17 June, which was the first day to begin operations, we have not been able to begin till the afternoon because we have spent the whole morning in the Sierra Leone Medical Council in Freetown; even when all the requested titles had been sent by mail, and the inscription forms had been properly filled in the Medical Council, we have had to go through a personal interview in order to confirm our ability. In that way we have had only 4 and a half days of work, which we have made good use of as far as we were allowed. In PH we had no time limit to work, still in CH we were first told that at 7 p.m. the health workers were leaving and so we could not operate from that time on. This time limitation in CH was extended in the last days with the hint that we could work from that time. This time limitation in CH was enlarged on the last days with the suggestion of giving some help in the shape of economic help for the operation theater staff, as it is apparently assumed habitually in this hospital and which has looked very strange to us.

On the whole we have been able to operate upon 126 patients of which 96 have been adults and 30 children; till the time of leaving, and reporting our direct communication with Dr. Fillie today there have been no mayor complications. The number of surgical procedures carried out has been 144, as in some patients 2 and 3 procedures had been carried out simultaneously (19 hidroceles and umbilical hernias).
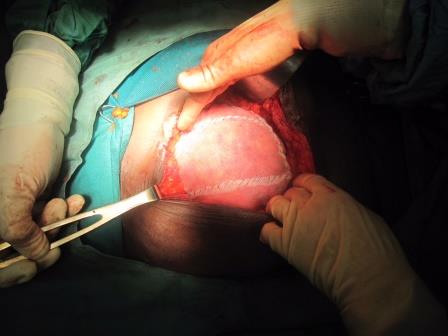
It is very important to stress that 70% of the inguinal hernias were H3 or H4 or more invalidating, as we have selected for treatment those that seemed more complex and more invalidating and required more time. On the last day of the mission we operated upon a giant goiter in a 12 year old girl with compressive complication which could not bear decubitum who was discharged the next day without any disphony or symptoms of hipocalcemia.
In spite of all the organizing problems that have troubled us, we can say that the campaign objective has been achieved, and from the view point of the number of patients operated upon the mission has been a success. The Police Hospital is a center where in the future new campaigns will be had because the interest of leaders and surgeons to collaborate with our foundations is maximal and the predisposition is absolute. It would be very interesting to be able to solve the problem of the sterilization of the material (they have no autoclave) and to dispose of another electric scalpel in order to make 100% use of the second operation theater they have. After 2 months I am keeping a periodical relation with Dr. Fillie and I believe it is worthwhile to work in this country habitually.
Dr. Cesar Ramirez