Host: Sisters of Nativity Hospital and Convent, Abuja Nigeria
Team members: Alan Kravitz, MD, Daniel Scarpetta, MD, Rony Ramia, MD Total cases: 126
Total patients: 117
Peds: 33
Background: The Sisters of Nativity (SON) Hospital and convent is located in Kamu, Nigeria. They provide primary care, OBGYN services, and some surgeries to their community.
Trip report: We arrived on the evening of November 9, 2024, after having flown into Abuja airport. We were met outside the airport by hospital staff, and brought to the SON compound. It is a 50 minute drive over good roads. We arrived at the convent to an enthusiastic welcome.
SON had done some publicity for this mission, so there were patients ready for surgery on Saturday, November 10. In addition, we were screening new patients both before the cases that day, and in between surgeries. Except for two patients with lipomas, all patients had either hernias, hydroceles, or testicle masses.
The adult inguinal hernia surgeries were done under local anesthesia. Pediatric cases were done with IV ketamine and diazepam, which was administered by a local physician. Selected adult patients were also given intravenous sedation, based on body habitus and nature of the hernia. One patient required a spinal anesthetic due to his obesity and large epigastric hernia.
All surgeries were performed in one operating room. We generally ran two tables in this room synchronously.
There were frequent power outages, but fortunately we were prepared and brought headlamps, which were always useful due to poor OR lighting. The surgical equipment was passable, but not excellent by any means. We had brought two small kits last year, and they were still there but missing some of the instruments. We also brought (and donated) two more surgical trays.
One of the advantages of this mission is that the accommodations in the adjacent convent are terrific. We each had our own room, complete with a bathroom and shower. The air conditioning (when functioning) and comfortable beds allowed us good sleep.
The sisters prepared our meals, and we ate breakfast, lunch, and dinner together every day. They were very gracious and generous hosts.
Sunday at SON is Sabbath: no work. This year we hung out and slept. Later in the afternoon our hosts drove us around the local environs on roads that were unpaved and barely passable, even in an SUV. We then went into Abuja and met with Dr. Austin Ella, who is a senior program manager with Caritas Nigeria, the official relief and development arm of the Catholic Bishops’ Conference of Nigeria.
On Monday we began seeing increasing numbers of patients for screening and surgery. Word of our mission had gotten out into social media and patients were lining up outside of the hospital. We actually became overbooked. There were communication issues with the workers at the front desk, who over-committed us. Throughout the week we often worked until 7 or 8 pm.
Many of the hernia cases were bilateral, recurrent, or incarcerated. Operating under straight local anesthesia (marcaine + lidocaine) is more tedious, and dissection needs to be more careful. We had no electrocautery available, though this wasn’t a barrier. Most inguinal hernia surgeries don’t bleed, and suture ligature of bleeding was needed only a few times.
We even fixed a large ventral hernia under IV ketamine anesthesia. The patients were uniformly grateful. Many of them had been experiencing hernia symptoms for years without
access to surgical care. In addition to hernia repairs, we removed several symptomatic lipomas, one orchiectomy, and many adult and pediatric hydrocelectomies.
After a busy week concluded on November 16, we returned home safely the next day.
It was a very productive week, and we are making plans for returning next year. There will be a focus on coordinating the schedule between the local staff and the surgeons so that we can start at 7 am and finish around 5 pm. We also have decided to limit our pediatric cases to greater than 5 years of age. Operating on smaller children requires fine dissection instruments, which we don’t have there. Also, many of these cases (hydroceles especially) are asymptomatic and potentially will resolve with time. And given the large need and our limited time in Abuja, a bigger social impact can be achieved by operating on symptomatic adults.
This was my second year at Sisters of Nativity, and we will return next year. It has many positive aspects: Very organized host organization, large numbers of patients who need surgical care, pleasant accommodations adjacent to our surgery location, good security, and easy access to an international airport.
Here is a link to the google photo album of our week in Abuja. It also includes some videos. https://photos.app.goo.gl/dceUZfEyuMZkDouP9
Report on Medical Humanitarian Mission to Fish Town, River Gee County, Liberia
Organizations: Organized by Liberia Physicians and Surgeons Without Borders (LPSWB) & Liberia Medical and Dental Association (LMDA)
Sponsor: Cllr. Kunkunyon Teh, Esq & Foundation
Date of Departure from Monrovia: October 31, 2024 Date of Arrival in Fish Town: November 3, 2024 Implementation Period: November 4 – 9, 2024
Team Composition
Team Member
Specialization/Role
Affiliation/Location
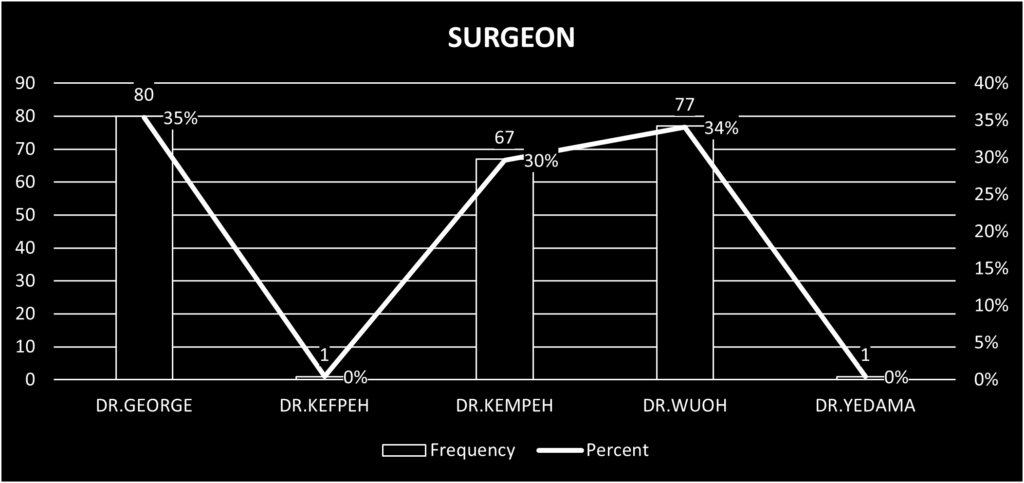
Dr. M. Peter George
Consultant General Surgeon, County Health Officer & Head of Department Surgery
Emirates Hospital, Gbarpolu County
Dr. Michael Kempeh
Specialist General Surgeon
J.F.K. Medical Center
Dr. Arthur Wuoh
Specialist General Surgeon, Medical Director
C.B. Dunbar Referral Hospital, Bong County
Dr. Levi Korheina
Specialist Anesthetic Physician, Medical Director
Liberia Government Hospital, Bomi County
Dr. Masuah Kokro
Specialist Family Medicine, County Health Officer
River Gee County
Dr. Luah Yardanmah
Specialist OBGYN, Medical Director
Fish Town Hospital
Dr. John T. Sarboah Jr.
Medical Officer
Military 14 Hospital
Dr. Wawakoh
Chief of Medical Staff
Fish Town Hospital
Roland Karnley
Certified Nurse Anesthetist
Emirates Referral Hospital, Gbarpolu County
Roger CorCor
Certified Operating Theater Scrub Nurse
Emirates Hospital, Gbarpolu County
J.F.K. Eye Department Team
Specialized Eye Care Services
J.F.K. Medical Center
This team comprised highly skilled professionals who collaborated to ensure the success of the six-day Community Outreach Eye Screening Program and Surgical Intervention in River Gee County.
Collection and Preparation of Materials
On October 31, 2024, all necessary materials and medical supplies were collected from Bunty Pharmacy at ELWA Junction by Dr. George, the team lead for the Liberia Physicians and Surgeons Without Borders (LPSWB). The following day, November 1, 2024, all materials were packed, labeled, and organized into four vehicles generously provided by our prime sponsor, Cllr. Kunkunyon Teh, Esq. Volunteers were informed to assemble at the A’la Lagune Resort between 12:00 am and 1:00 am for departure.
2. Departure and Initial Journey
The team departed from Monrovia at 2:44 a.m. on November 2, 2024, and arrived in Ganta, Nimba County, at 5:16 a.m. There, the vehicles made a brief stop for refueling. Unfortunately, no food options were available for volunteers at that time, so we continued our journey.
3. Rest and Meals in Saclepea
We reached Saclepea, Nimba County, at 7:27 am, where food was purchased for the team. Fifteen plates of food, including pepper soup, “rice and beans,” and a local dish “GB,” were served to the team. We departed from Saclepea at 8:15 am. Between Saclepea and Tappita, we encountered a major obstacle: getting stuck in the mud.
4. Challenges En Route to Zwedru
After overcoming the muddy stretch, we reached Tappita at 11:24 am and arrived in Nellah Town by 12:42 pm, where commercial trucks were also stuck. The truck drivers assisted us in moving forward, recognizing our mission’s humanitarian purpose. We entered Grand Gedeh County at 1:26 pm, where we went through immigration, and shortly afterward, we encountered another delay in Glodialialy Town, getting stuck from 2:16 pm to 5:45 pm. During this delay, one of our vehicles, with plate number A64679, suffered a fuel tank issue. We arrived in Zwedru City at 8:33 pm and met with Dr. Manneh, the Medical Director of Martha Tubman Memorial Hospital, who kindly hosted our team.
5. Vehicle Servicing and Continued Journey to Fish Town
On the morning of November 3, 2024, our vehicles were taken to a local garage in Zwedru for servicing and necessary repairs. Departed from Zwedru at 11:52 am on a smoother road and reached Kaloken, the commercial hub of River Gee County, at 1:39 pm. By 3:30 pm, we arrived in Fish Town, where we were warmly welcomed by Dr. Masuah T. Kokro, County Health Officer, and the local chief elders of Fish Town, which took 4 hours. We visited Fish Town Referral Hospital that evening to set up the operating room and arrange our surgical materials, and we were welcomed by the hospital administration led by Dr. L. Yardanmah, Medical Director of the Fish Town Hospital, River Gee County.
6. Commencement of Medical and Surgical Activities
On November 4, 2024, we began our medical mission at Fish Town Referral Hospital, which included:
Surgical procedures
Medical consultations
Ophthalmology screening exercises
We were able to treat numerous cases, providing essential medical care and surgical interventions to the local community.
7. Strike by Nurse Anesthetists and Impact on Services
On November 8, 2024, the Nurse Anesthetists went on strike, significantly affecting the pace of surgical cases, as we only had one anesthesiologist available. This disruption caused delays, but the team continued to provide services as efficiently as possible.
Patient Data Analysis.
Ophthalmology Patients Data Analysis
Summary of Cases
Number of Cases
Cataract
93
Glaucoma
12
Pterygium
45
Corneal Scar
20
Refractive Error
312
Dry Eyes
42
Total Patients Screened
524
Additional Outcomes
Number
Patients Referred
170
Glasses Dispensed
301
Not Received Glasses
11
Normal Patients
42
Surgical Patients Data Analysis
Conclusion
The Medical Humanitarian Mission to Fish Town, River Gee County, was a resounding success, demonstrating the impact of collaborative efforts among skilled medical professionals, local healthcare providers, and generous sponsors. Over the course of the mission, the team provided essential medical, surgical, and ophthalmological services to the underserved population of River Gee County. With no logistical and operational challenges, only including delays en route and a temporary strike by Nurse Anesthetists, the team remained committed to delivering high-quality care.
The outreach served 524 ophthalmology patients, with 301 pairs of glasses dispensed and 170 patients referred for further care. The surgical and medical consultation services offered by the team addressed numerous complex cases for 277 patients, contributing significantly to the health and well-being of the local community.
This mission highlighted the critical need for sustained healthcare interventions in rural Liberia and underscored the importance of multidisciplinary collaboration to overcome barriers to healthcare access.
Recommendations
Strengthen Local Healthcare Systems
Provide additional training for local healthcare staff, including Nurse Anesthetists, to ensure continuity of care even during emergencies or strikes.
Establish mentorship programs for local medical professionals to enhance surgical and medical capabilities.
Expand Medical Outreach Programs
Continue organizing similar humanitarian missions in other underserved regions of Liberia.
Develop a structured schedule for periodic medical outreach activities to ensure consistent healthcare delivery.
Enhance Logistics and Support
Secure reliable transportation and backup vehicles to avoid delays caused by breakdowns during missions.
Increase pre-departure planning and support to minimize challenges en route to remote areas.
Strengthen Community Engagement
Collaborate closely with local leaders and health authorities to better understand the community’s healthcare needs.
Promote health education campaigns to increase awareness of preventable conditions such as cataracts, glaucoma, and refractive errors.
Sustain Funding and Partnerships
Seek additional sponsorships and partnerships to support future missions, including equipment procurement, medications, and supplies.
Foster long-term relationships with donors and sponsors to ensure sustainable funding for outreach initiatives.
Monitor and Evaluate Impact
Establish mechanisms to collect data and evaluate the impact of outreach missions, focusing on patient outcomes and community health improvement.
Use these evaluations to refine future outreach strategies and enhance service delivery.
Prepared By: Dr. M. Peter George, MD, FACS Team Lead, River Gee Medical Humanitarian Mission Liberia Physicians and Surgeons Without Borders (LPSWB)
HERNIA INTERNATIONAL 2024 MONGOLIA TEAM & THE SECOND GENERAL HOSPITAL MONGOLIA
JOINT WORKSHOP REPORT
2024.09.25 Ulaanbaatar city
Our workshop, which has been a tradition for more than 10 years, was organized for the 11th time this year. The joint team of 8 Australian and Mongolian surgeons from the Hernia International Hernia Foundation and the Second General Hospital of Mongolia worked from September 9th to 13th at the Central Hospital of Govisumber Province under the guidance of Professor Bohdan Smajer from the UK, a member of Hernia International, and Dr. Ts. Narmandah, Honorary Doctor and Consultant Physician of the Second State Central Hospital. The joint team led by Professor Richard Turner continued the workshop at the Surgical Department of the Second State Central Hospital from September 16 to 20. The theme of the training was “Modern trends in hernia surgery” and it included both theoretical and practical parts.
Theoretical training was conducted in small groups every day after the surgical treatment, and interview training was conducted on each case. The 16 hours of lectures on the following topics such as “Global trends in hernia surgery”, “Anatomy of various hernias”, “Hernia surgery”, “Botox treatment options for hernias”, “Surgery for complications of hernias”, “Mesh selection for hernia surgery”, “Laparoscopic techniques of hernia repair” were given to the participants. During the workshop, 16 hernia cases were performed at Govisumber Central Hospital and 21 cases were performed at Second General Hospital, making a total of 37 cases of various hernia repairs.
The training was attended by surgeons and nurses from SGH, Govsumber Aimag Central Hospital, Darkhan-Uul Aimag Central Hospital and central hospitals of Nalaih, Baganur, Bayanzurkh, Sukhbaatar districts and also from private hospital in Ulaanbaatar city. 25.09.2024
As part of the training, members of the International Hernia Foundation donated a laparoscopic surgery training unit to the Department of General Surgery of SGH of Mongolia.
Photo 2. While a lecture was being given at the Gobisumber Central Hospital
Photo 3. Hernia International and the Second General Hospital Team with the Management Team of Gobisumber Central Hospital
Photo 4. Round
Photo 5. On-site training with Dr. Enkhtogtokh
Photos from the Workshop at the Second General Hospital
Conclusion
This training was as effective as previous years, and doctors were taught new techniques and principles, BOTOX treatment methods, the importance of hybrid cages, and eTEP treatment. At the end of the training, our doctors were able to freely exchange knowledge and information by asking questions they were interested in.
The report was written by:
Z. Sonor /Colorectal Surgeon, Department of General Surgrey, Second General Hospital of Mongolia/
Reviewed by: Ts. Narmandakh /Honored Doctor of Mongolia, Consultant Surgeon, Second General Hospital of Mongolia/
– On the 14th of September 2024 most of the Cirujanos en Acción team left Madrid for Lima at 5pm, bringing medical and biomedical material in sufficient quantity to cover the objectives of the campaign, as well as 2 diathermy generators from the Foundation
– On Sunday 15th September at 06:00 hours, the team arrived at Jorge Chavez Airport and was welcomed by a small local entourage. That same day, the evaluation of the patients began in the morning at the Ventanilla Hospital, by Dr. Concha Bernardos (Vascular Surgery) and Dr. Jose Maria Pérez Alfranca (General Surgery).
– Surgical activities started on Monday 16th September, as detailed below.
– The surgical activities culminated on Friday 27th September with a closing ceremony organized by the Regional Health Directorate of Callao.
– On the evening of 28 September, most of the team left Jorge Chavez airport for Madrid.
1.2 ADULTS PACIENTS:
During the health campaign, 159 patients and 193 cases were operated on. Of the total, 86 patients (93 cases) were treated for hernias and 73 patients (100 cases) for varicose veins in the lower limbs.
The type of intervention performed was hernioplasty and/or eventroplasty, with the polypropylene prosthesis being placed. In the case of umbilical hernias, the decision to use a polypropylene prosthesis was based on the size of the ring. The hernia pathology operations were performed in 02 operating theatres, with 2 anaesthesiologists and 2 surgeons in each theatre.
– Number of adults: 86
– Number of procedures performed: 93.
– Average number of procedures per day: 10.
With regard to surgery for varicose veins in MMII, phleboextraction of the internal saphenous vein was performed using the scripting technique in most cases. In the rest, external saphenous ligation or perforating ligatures were performed. In addition, phlebectomy of the varicose bundles was performed in all cases. Varicose vein operations were performed in 02 operating theatres, with 2 anaesthesiologists and 1 surgeon.
PHLEBOEXTRACTION OF INTERNAL SAPHENOUS VEIN 94 CASES
EXTERNAL SAPHENOUS VEIN LIGATION 4 CASES
PERFORATOR LIGATION 2 CASES
TOTAL 100
1.5 Total pacients
HERNIA AND ABDOMINAL WALL SURGERY: 86 PATIENTS.
VARICOSE VEIN SURGERY: 73
TOTAL NUMBER OF PATIENTS: 159.
1.6 COMPLICATIONS
Serious:
There were no acute complications during the first 24 hours post-operatively.
Recurrent:
As of today that we are in contact with Dr. VELASQUEZ to follow the evolution of our patients, we have not received any information of complications so far.
CAMPAIGN REPORT
2.1. THE PLACE
Last September, a new cooperation campaign took place in the district of Ventanilla (Callao – Peru). Ventanilla is located 34 kilometres northwest of Lima and is a coastal district with a constantly growing population of 355,830 inhabitants. Its main independent economic activity is commerce, ecotourism-recreational activities and, to a lesser extent, artisanal fishing.
The Ventanilla Hospital began its activities in 1964 as a health centre in a building on 12th Street in the Ciudad Satélite de Ventanilla housing estate. On 8 February 1967, it moved to its current location on block 3 of Avenida Pedro Beltrán, next to the Ventanilla Police Station. Since January 2013 it has functioned as the Ventanilla Hospital, with Dr. David Pablo González Sáenz as its first Director, and is currently under the direction of Dr. Hamilton Alejandro García Díaz.
Ventanilla hospital has 5 operating theatres, 4 of which were available for the campaign, initially 2 operating theatres for abdominal wall pathology and 2 operating theatres for varicose veins. The surgery area has an inpatient ward, which was used for patients who required monitoring for more than 1 day or for some particularity of the patient.
The recruitment of the patients took place a few days before the campaign and was carried out by the medical staff of the Ventanilla Hospital. On Sunday 15th September the patients were evaluated by Dr. Concha BERNARDOS (Vascular Surgery) and Dr. Jose Maria PEREZ (General Surgery). This evaluation consisted of prioritisation according to the patient’s individual situation and assessment of the need for surgical treatment.
The project of this campaign aimed to treat between 90 to 100 patients, at a rate of 15 to 20 patients per day. At the end of the campaign, 159 patients were operated on and 193 surgical procedures were performed.
For this campaign we also had the support of Hernia International, who lent the Ventanilla Hospital four (04) boxes of surgical instruments, which made it possible to perform the surgeries continuously in multiple operating theatres.
2.2. THE TEAM
The team of volunteers consisted of 5 general surgeons, 1 vascular surgeon, 2 vascular surgery residents, 3 anaesthetists, 5 nurses and a 3rd year medical student:
– A general surgeon from the Hospital Regional Policial de Arequipa (Dr. Ameth Alvarez).
– A general surgeon from Australia (Marisol Perez Cerdeira).
– A general surgeon from Spain (José Maria Perez Alfranca).
– 2 general surgeons from Lima (Roberto VEGA, Ronal Medina).
– A vascular surgeon from Spain (Dr. C Bernardos). Spanish team coordinator.
– 2 vascular surgery residents from Spain (Beatriz García Nieto and Alejandra Vázquez).
– 3 anaesthesiologists from Spain (Pilar Murga Pascual, M Jesús Sánchez Colomer, Fernando Carbó).
– 4 nurses from Spain (María José Fornier Coronado, María Jesús Nieto Berrocal, Lucía Ruiz Arasanz y Maria Alicia Zapata Piquer)
– 1 nurse from Arequipa (Giovanna Haydee Mesa Mendoza de Álvarez)
– 1 field worker in Lima (Martha Vasquez)
– 1 medical student (Paloma Baselga).
2.3. LOCAL STAFF
– 01 general surgeon coordinating recruitment (Dr. Velásquez)
– 04 general surgeons from Ventanilla Hospital (Bernal, Cutipa, Lavado, Huamani)
– 04 general surgery residents from Ventanilla Hospital (Alice Bada, Pedro Anderson, Mildret Rodriguez)
– Nurses and technical staff from the surgical centre.
2.4. EQUIPMENT
The following equipment was available for this campaign:
– 4 daily operating theatres with operation from 8-20h or until the schedule is completed.
– Anaesthetic recovery with 6 beds.
– An Echo Doppler for pre or intraoperative evaluation.
– 2 diathermy generators from Ventanilla Hospital and 2 diathermy generators brought by Surgeons in Action.
SURGICAL INSTRUMENTS
For the present campaign we had 4 boxes of instruments from Ventanilla´s Hospital and 04 boxes from Hernia Internacional, each box to be used and sterilised with a minimum content of:
– 02 FARABEUF OR 2 ROUX
– 10-12 MOSQUITOES
– 2-3 CRYLES
– 1 MAY SCISSORS
– 1 METCENBAUM SCISSORS
– 2 TWEEZERS WITH TEETH
– 2 DISSECTING FORCEPS
– 1 NEEDLE HOLDER
– 1 SCALPEL HANDLE º4
– 4 FLEBOEXTRACTOR CRABS AND HOOKS (brought by Surgeons in Action)
2.5. ANAESTHESIA
Type of anaesthesia used:
– SPINAL. 126 PATIENTS.
– LOCAL AND SEDATION 26 PATIENTS.
– GENERAL
3 PATIENTS
2.4. ASEPSIS AND SURGICAL SUPPLIES
The following surgical material was brought for this campaign according to the following list:
2.5. OUR LIFE ON……
The Ventanilla Hospital is located in the district of the same name, and it is a 50-minute drive from the Lauritas Sisters’ place of residence, Casa de reposo, to the hospital and back, in a vehicle available only to the team.
The month of September was cold in the mornings, which was the constant on arrival at the hospital. By lunchtime, which was at 02:30 pm, the weather changed to a little sunny, which improved our spirits..
Between surgeries, there was always time to share with colleagues and also with the residents, who were the ones who gained the most interaction and experience during all the days of the campaign. At the end of each surgery, the feeling of satisfaction at having achieved the objectives of the campaign was evident in the team. The activities of the surgical act were not left aside, with the preoperative evaluation and the operative report being carried out by the surgeon in charge of the procedure. During the course of the campaign there were some pleasant moments not associated with the operating theatre, such as the visit of a dance group, who showed us a little bit of Peruvian folklore, making the surgical team participate in this activity, which was very pleasant for everyone. Also during the course of the campaign, Dr Roberto ESPINOZA ATOCHE – Regional Director of Health of Callao, visited us and showed his gratitude to the team for the activity, highlighting their generosity, solidarity and great surgical capacity.
At the end of the campaign there was a closing activity, which was presided over by the Regional Health Director of Callao, with the presence of the Director of Ventanilla Hospital, in this activity once again thanking the selfless work of the team with the sole objective of improving the health of the people of Ventanilla most in need. The closing ceremony also included the presentation of certificates to the members of the Surgeons in Action team, a fact that was highlighted in the local media and virtual media of DIRESA Callao..
In the free time there was time to get to know part of Lima, such as the districts of Barranco and Miraflores, with all their architecture, culture and traditional food. There was also time to get to know a little more of Peru, with a short visit to Ica, Nazca and Paracas..
– Ventanilla Hospital has 4 rooms available for campaigns, 2 operating theatres complete with anaesthesia machine and 2 smaller operating theatres suitable for low complexity procedures, which do not have electrocautery.
– Ventanilla Hospital has a dining room where staff can have lunch.
– The Ventanilla Hospital has surgical residents who are very supportive of the campaign.
– The nursing staff of the surgical centre has experience in conducting these campaigns, successfully managing the flow of patients in the surgical centre and in the hospital.
– Ventanilla Hospital has its own sterilisation centre.
3.2. Improvements objetives:
– Recruitment of patients earlier, for greater coverage.
– The leader of the local campaign team should be a surgeon from the hospital or centre where the campaign will take place.
– Manage the actual number of beneficiaries of the campaign in order to better distribute the patients and the surgical team.
– The location of the team’s accommodation should be closer to the place where the campaign will take place, in order to avoid transport time, which is made worse by the high traffic in Lima.
Comprehensive Report on the Outreach by Liberia Physicians and Surgeons Without Borders (LPSWB) in Collaboration with Hernia International UK at Bongmiles Hospital, Bong County, Republic of Liberia (26th–29th September 2024)
Introduction
From 26th to 29th September 2024, a team from the Liberia Physicians and Surgeons Without Borders (LPSWB), in collaboration with Hernia International UK, conducted a medical outreach at Bongmiles Hospital, Bong County, Republic of Liberia. The mission aimed to provide essential surgical care, focusing on hernia repairs and other general surgeries pathology to underserved rural communities. The outreach was facilitated by a team of highly skilled professionals from diverse specialties, committed to addressing the health needs of rural Liberia.
Team Composition
The outreach team included the following professionals:
Dr. M. Peter George – Consultant Emergency, Rural, and General Surgeon
Dr. Ayun Cassell III – Consultant Urology Surgeon
Dr. Michael Kempeh – Specialist General Surgeon
Dr. Onyekachi C. Subah – Specialist Transfusion Medicine & Public Health
Dr. Seanan Subah – Specialist General Surgeon
Dr. Arthur Wouh – Specialist General Surgeon
Dr. Liveah Koheneh – Specialist Anesthetics Physician
Dr. Ambrous Fawenel – Medical Officer in Surgical Training
Dr. Younda – Medical Officer on Rural Surgical Rotation
Dr. Alexandra Tokpah – Medical Officer/Medical Director of Bong miles Hospital
Mr. Eric Cassell – Strategist and Financial Adviser
Roger Corcor – Certified Scrub Nurse
Momoh Sonnie – Certified Nurse Anesthetist
Objectives:
The primary objective of the outreach was to provide life-saving surgical interventions, primarily focusing on hernia repairs and other general surgical procedures, in a rural setting. Additionally, the team sought to:
Alleviate the backlog of surgical cases in the region.
Provide postoperative care and education.
Train local medical staff to enhance surgical capacity in rural Liberia.
Arrival and Preparation
The team arrived at Bongmiles Hospital on the 26th of September 2024 and immediately began preparations for the surgeries, including patient evaluation, resource allocation, and surgical setup. The surgeries commenced on the 27th of September and continued through to the 29th.
Dr. Alexandra Tokpah and Dr. Younda were responsible for patient recruitment, ensuring all candidates for surgery were appropriately screened and diagnosed. They worked in collaboration with the local hospital staff to ensure seamless coordination.
Data Collection and Analysis
Throughout the mission, patient data was meticulously collected for later analysis. The following parameters were documented:
Patient Diagnosis
Gender Distribution
Type of Procedures Performed
Surgical Outcomes
Postoperative Care
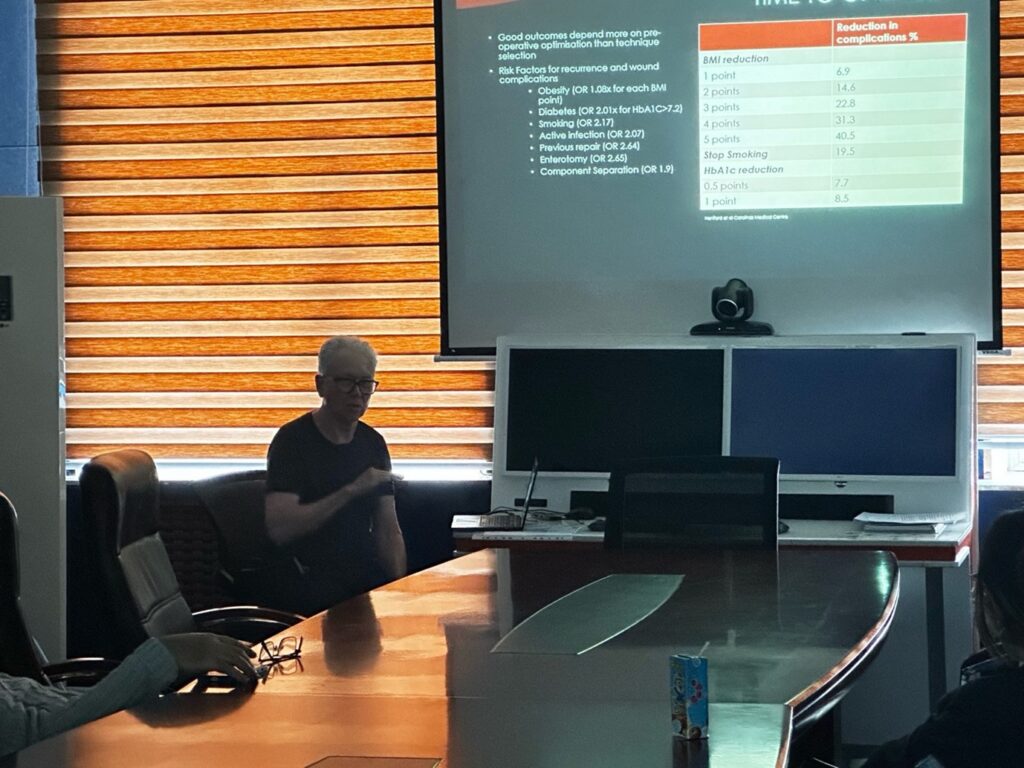
Anesthesia Given
Diagnosis Percentage Breakdown
Procedures Performed by Each Surgeon
Analysis of Findings
Patient Diagnosis
Patients were screened and diagnosed for various conditions, primarily focused on hernia repairs. Other diagnoses included hydrocele, lipoma, and soft tissue masses.
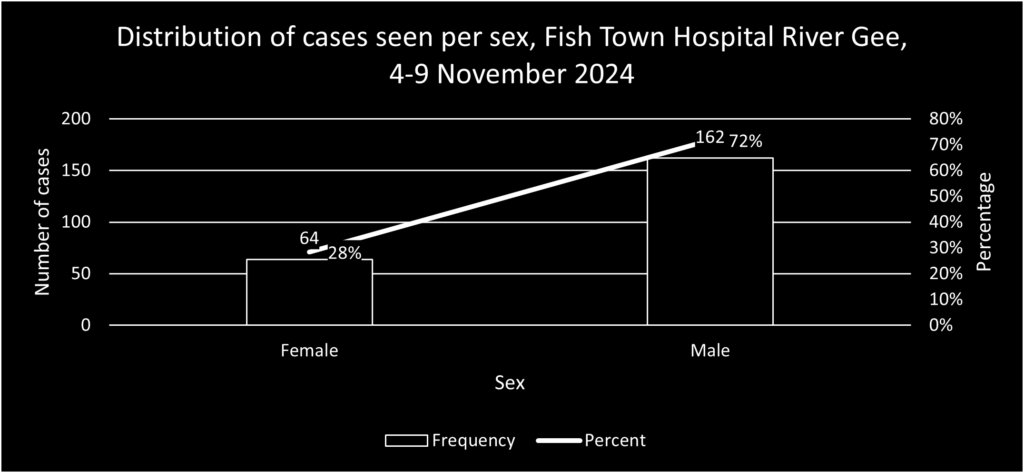
2. Gender Distribution
Male: 81%
Female: 19%
The significant gender disparity reflects the prevalence of hernias in male patients.
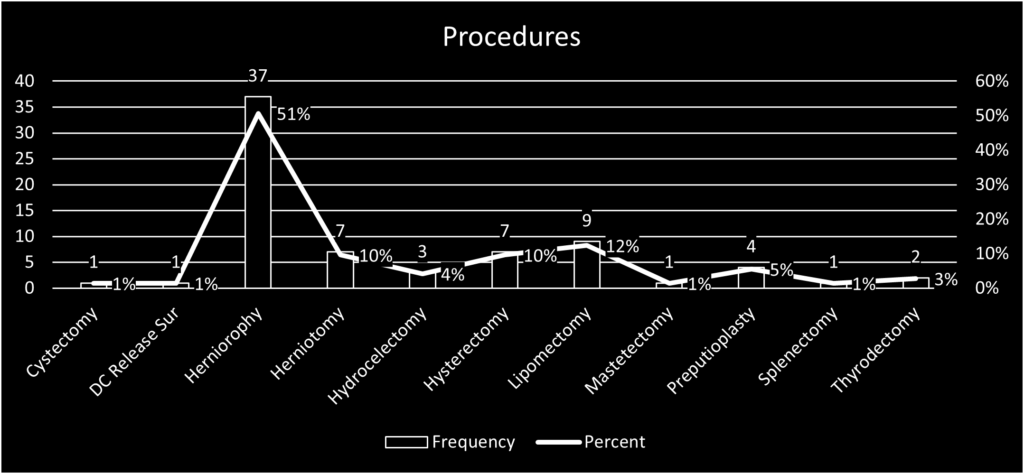
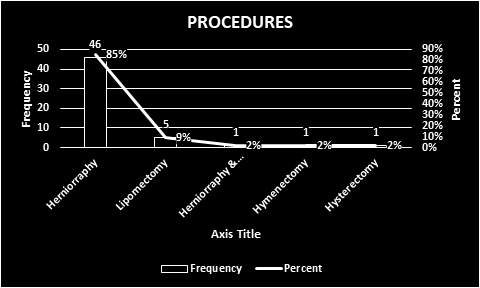
3. Type of Procedures Performed
The majority of surgeries were hernia repairs. Other surgeries included:
Hydrocele repairs
Lipoma excisions
Soft tissue mass removals
4. Surgical Outcomes
Successful Surgeries: 100% of all surgeries had a positive outcome with no complications reported.
Complications: No complications were noted.
5. Postoperative Care
The postoperative care team, led by Dr. Liveah Koheneh and Momoh Sonnie, ensured that patients received appropriate pain management, wound care, and follow-up consultations. No cases of postoperative infection were reported after 2 weeks.
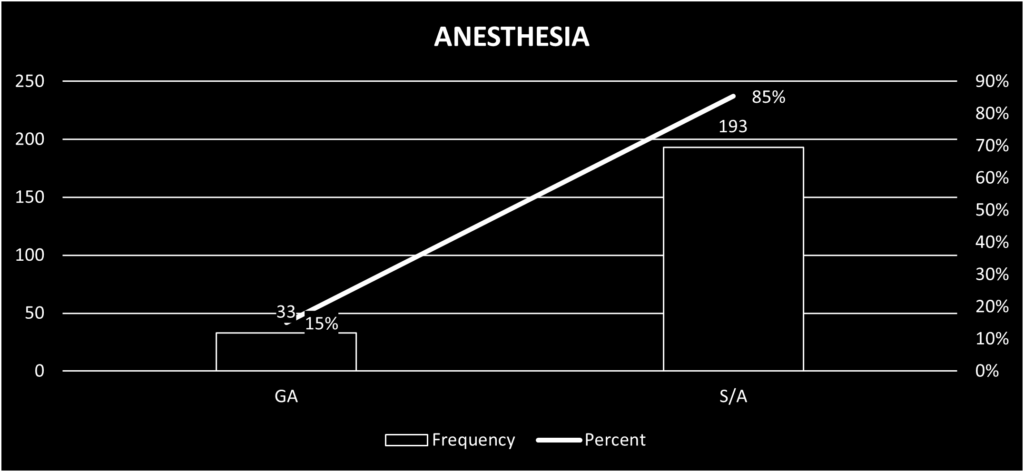
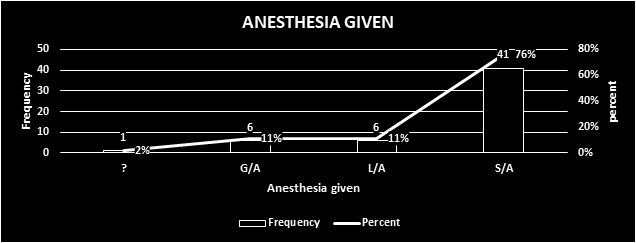
6. Anaesthesia Given
Dr. Liveah Koheneh, the Physician Anesthetists, was responsible for administering anesthesia. The procedures were carried out under:
Local anesthesia: 11%
Spinal anesthesia: 76%
General anesthesia: 11%
Unknown: 2%
The choice of anesthesia was based on the type of procedure and the patient’s condition.
7. Procedures Percentage
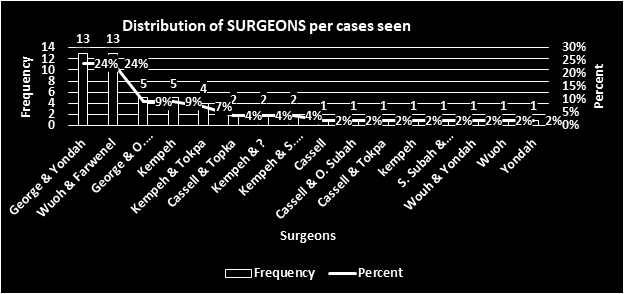
9. Procedures by Doctors
The above distribution highlights the contribution of each surgeon to the success of the outreach.
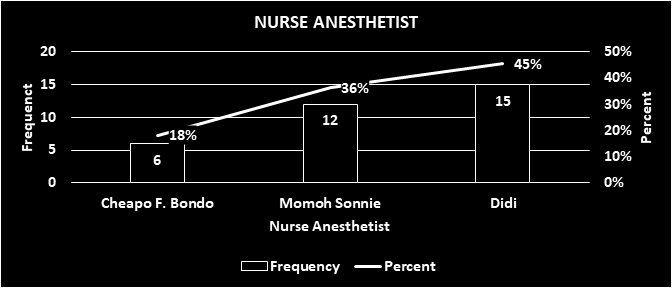
10. Nurse Anaesthetics
Conclusion
The medical outreach at Bongmiles Hospital was a resounding success. The collaboration between Liberia Physicians and Surgeons Without Borders and Hernia International UK resulted in the successful treatment of numerous patients, many of whom had been waiting for surgical intervention for months. The outreach not only alleviated the surgical backlog in Bong County but also provided valuable training and experience for local medical personnel.
Recommendations
Continuous Outreach: There is a need for ongoing surgical missions to rural areas to address the unmet surgical needs.
Capacity Building: Training local healthcare providers will enhance their ability to handle such cases independently.
Data Utilization: The collected data should be used to plan future outreaches and improve resource allocation.
Post-Operative Follow-Up: Future outreaches should incorporate long-term follow-up plans to monitor patient recovery.
The outreach team would like to extend their gratitude to Hernia International UK, Bongmiles Hospital,Ministry of Health ,Liberia Medical and Dental Association LMDA and the local community for their support in making the mission a success.
Total procedures 2 Total patents 2 COMPLICATIONS: 2 CAMPAIGN REPORT 3 THE PLACE 3
THE TEAM 3
THE LOCAL STAFF 4 THE EQUIPMENT 4 ANAESTHESIA 5
ASEPSIS AND SURGICAL MATERIAL 5 OUR LIFE AT DANGBO 6 CONCLUSION 7
Strengths of this place: 7
ObjecAves for improvement: 7 BUDGET: (small breakdown of costs) 8
COST PER PARTICIPANT: 8
TOTAL COST OF THE CAMPAIGN: 8 SIGNATURES 8
1. TECHNICAL REPORT:
1. DATES AND LOGISTICS DEPLOYED:
The Surgeons in Action Foundation (SAF) has deployed a team of 9 volunteers to carry out a campaign in Benin, at the Hopital Albergue d’Amour Redemptour in Dangbo.
We had 7 members from Madrid and 2 from Zurich on the 28th of September 2024, meeting in Paris. In total, we have transported 200kg of medical material for the campaign, including 23 medicines with export authorisation no. 37587/24 from the AEMPS.
The journey to Dango is reasonably good. The flight, with Air France, via Paris, takes about 10-12 hours depending on the connection. From the airport to Dangbo it is about 2 hours by car, which we have in two vans organised by Sister Opportune.
It is important to note the issue of luggage. Air France allows a 23kg baggage allowance. They are strict about the weight, and, more importantly, they have been quite strict about the weight. importantly, they gave us a lot of trouble in Cotonou to check in some of the bags we were bringing (electrodiathermy and harmonic generator). For future SAF campaigns, I think it is important to stop carrying ‘Chinese’ bags, which are becoming more and more problematic at airports and the airlines do not allow us to check them in. They will have to be replaced by more robust travel cardboard boxes.
We worked at the hospital from 29 September to 5 October inclusive.
The return trip to Madrid and Zurich took place on 6 October 2024.
2. ADULT PATIENTS:
80 surgical procedures have been performed on 75 patients. An excel file with the complete database is ajached.
Breakdown by pathology: 10 total thyroidectomies 16 hemithyroidectomies
37 inguinal hernioplasties (Lichtenstein), 4 of them bilateral. 3 midline hernias (Rives)
No paediatric patints were treated in this campaign.
Totalprocedures
80
TotalpaJents
75
COMPLICATIONS:
1 patient with immediate surgical reoperation for cervical haematoma. The patient developed a cervical haematoma during anaesthetic awakening. Reintubation, exploration of the surgical field, and haemostasis were performed without further incident.
patient had an intraoperative haemorrhage of about 700cc during a difficult total thyroidectomy. The postoperative course was unevenful.
patients with inguinal hernioplasty developed a haematoma in the surgical wound, which was treated conservatively, with good evolution after our departure.
2. CAMPAIGN REPORT
THEPLACE
Hopital Albergue d’Amour Redemptour in Dangbo is a location that SAF has been very familiar with f many years, regularly conducting campaigns. This hospital, run by Sister Opportune, maintains constant activity of collaboraAon with different organisations, which allows them to carry out surgical campaigns in their hospital on a regular basis. Our campaign was the seventh this year at the centre bringing the total to ten by the end of the year.
Dangbo is a small town in southern Benin, an hour’s drive from the capital, Portonovo, and about ten hours from Cotonou airport. It has a central area, crossed by the dirt road that connects it to the rest the country, where the most important part of the town lives in small buildings. It has a market, which we were only able to visit on Sunday afternoon after work, when it was empty. The rest of the village made up of houses scattered around the countryside.
It has a hotel, the Behova Hotel, where we stayed in reasonable comfort. It has air-conditioned rooms with cold running water. It also has a small restaurant where we had breakfast daily.
The hospital consists of a group of small single-storey buildings within a fenced enclosure.
Our activity has been developed in a small surgical block, which has an operating theatre in which we have arranged two surgical tables. It also has a small cleaning and sterilisation room, a room used for storage, and an entrance that serves as a post-anaesthetic recovery room. The adjoining building houses the hospital wards. In the style of other places in Africa, they are open-plan rooms with bed where patients and their families spend time from the time they arrive unyil they are discharged.
In this area there is also the house where the nuns live in community, which is where we have had a daily lunch and dinner, generously served by them, with impressive affection and dedication.
Another building is used for outpatient consultations. For our campaign, Sister Opportune had previously selected the patients we were going to operate on, with a solvency and organisation that unusual in other locations we work with .It was only necessary to use Sunday morning to consult all the patients and organise the surgical plan for the whole week. All the patients have a small folder with the medical history, with a brief description of their medical history, clinical diagnosis, and medications. Some patients bring an imaging test performed in the capital.
THE TEAM
The team is made up of 2 nurses, 4 surgeons, 2 anaesthetists and 1 biomedical engineer: David Fernández Luengas: Team coordinator. Surgeon.
Sandra del Barrio Anaya: Surgeon. Ana M Gay Fernández: Surgeon.
Silvestra Barrena Blázquez: Nurse. Michael Wentkowsky: Engineer.
It is very important to highlight the good atmosphere in which our activity and coexistence has developed. This is undoubtedly due to the enormous human quality of the members of the group, to their great professional training.
The language barrier between Katharina and Michael, volunteers from the NGO Hernia International northern Swiss, German-speaking and fluent in English, and the rest of the Spanish team, has been overcome thanks to the collaboration of all. Michael’s fun and open attitude is very remarkable, as he has constantly encouraged has constantly encouraged the group, favouring that connection, sometimes difficult when the largest part of a group speaks a different language. The collaboration with Hernia International is very important for the SAF, and it is great news that, once again, a joint team has developed a campaign in such a good working atmosphere. I think K&M have learnt more Spanish than we have learnt English!!! Katharina and Rocío worked very well together to perform the general and spinal anaesthesia, and brought a lot of security to the team. All patients have received anaesthetic treatment of the highest quality.
The team of surgeons worked very closely together, in alternating pairs that allowed us to share our work with each other. We have performed some fairly complex procedures in a good atmosphere of collaboration, and we have been very effective in achieving the planned plan of interventions, at a very high pace.
Silve and Nuria have worked very hard in the operating theatre, from organising the material, circulation and instrumentation in the operations, supporting the anaesthetists and taking care of the patients in the pre- and immediate postoperative period.
Michael, a biomedical engineer who always accompanies Katharina on the campaigns, has carried out repairs on several devices in the operating theatre (notably the repair of two monitors for intraoperative control), and has been appointed Celador Jefe of the team, thanks to his great willingness for all the tasks we have asked him to carry out.
LOCALSTAFF
The daily work on this campaign would not have been as effective if we had not been able to count on the collaboration and hard work throughout the week of the hospital’s local team.
First of all, Sister Opportune, the real heart and soul of the hospital. She has been responsible for the recruitment of patients, and for organising all the activity of the hospital so that we could work at such a high pace.
Her colleagues in the community have taken care of us during the lunches and dinners, which they have prepared for us with great dedication, even late at night, as we have finished several days later than 22h. Our thanks to Nadine for taking such good care of us.
Gavin, the nurse, spent the whole week at the hospital, with full dedication to the operated patients, helping us with dressings, medication and communication with the patients.
Silvie, Filomene, Protector and worked alongside us in the operating theatre, developing a very efficient activity of patient flow, cleaning and sterilisation of material and operating theatre.
This place has many advantages for the realisation of surgical campaigns, but its greatest strength is undoubtedly its human team.
THE EQUIPMENT
Expendable material: We have used all the material we brought with us, about 200kg. The hospital has a lot of material that has been contributed by previous campaigns, well organised and handy in the warehouse, which we have tried not to use. There are disposable surgical drapes, sutures, various operating theatre materials. There are also cloth pyjamas and clogs which are washed daily.
Surgical equipment: There are 3 electrosurgical units in good working order (Michael did some repair work to get them in good working order). Michael tried to fix a fourth device (Valleylab) but it is beyond repair. In any case, with these three devices, we can work perfectly well.
We also brought an ultrasound generator for the thyroid surgery, loaned by the company Medical Cañada, with enough consumable forceps for all the procedures.
Anaesthesia: We used a Drager Fabius ventilator which had been repaired in the weeks prior to our arrival, and which worked correctly, with no problems. There is no capnograph. There are two vital signs monitors, which Michael managed to repair and get working. We have used portable pulse oximeters brought by us, a portable automatic blood pressure cuff and a portable infusion pump. On the day we were leaving, the new Mindray WATO EX-35 ventilator arrived, which has been funded by the Bisturí Solidario FoundaAon and the Asociación Infancia y Cirugía en Dangbo. It has already been installed and can be used in the coming campaigns. It is a great leap in quality, firstly because it is more modern and complete than the other ventilator, and secondly because it will allow us to have two general anaesthesia stations.
ANESTHESIA
During the Campaign we performed 26 thyroidectomies under general anaesthesia, with orotracheal intubation, mostly using 7.5 tubes (almost all patients were women). On 4 occasions we used a Mcgraph video laryngoscope, which we carried specifically for this purpose, due to the expected difficulty in the airway. No awake patient was intubated. We did not have capnography or an oxygen sensor, although we did measure volume curves. We had several filters that changed colour on contact with CO2, useful for checking correct intubation in case of doubt.
Approximately half of the cases were performed with Sevorane, there are several bojles there, and the other half with percussion of propofol in an infusion pump that we carry.
We also performed 3 general anaesthetics with a laryngeal mask, for a fibroadenoma and 2 large lipomas.
There were 2 local anaesthesias with sedation for neck lipomas, and the rest of the anaesthesias (44) were spinal, for inguinal, umbilical and epigastric hernias. For the larger, isobar bupivacaine had to be used.
Patients operated under general anaesthesia stay 1-2 hours in the room next to the operating theatre, on a stretcher that allows for some back support (although it is in poor condition) with a pulse oximeter and oxygen when necessary. Silvie and Filomene helped us to keep an eye on them. We took almost all the material we used ourselves, and left what we had left over there. It is worth noting that there is a large amount of hyperbaric bupivacaine and levobupivacaine. We also left about 40 bojles of cefazolin 2g, and 5 bojles of clindamycin 600mg. We left over 20 ampoules of propofol and 10 bojles of 50 ml 2%. The 45 ampoules of fentanyl that we did not use were left with Soster Opportune for safekeeping. As for monitoring, despite Michael’s help with the arrangement of 2 monitors that have EKG, pulse oximetry and blood pressure, more need to be carried. The cuffs are badly damaged and leak or fail constantly. Also, for the patients we left on the stretcher outside, there is no monitoring. We carried 3pulse oximeters and a portable automatic blood pressure cuff which helped us a lot.
ASEPSIA AND SURGICAL MATERIAL
Instruments: For this campaign we have brought 5 boxes of instruments from the SAFA, two for thyroid and 3 for hernia. We also used instruments available in the hospital, which are in a reasonable state of conservation, although they are very limited. This allowed us to have a quick rotation, which is essential to be able to operate on an average of 15 patients per day.
They have a small autoclave machine (Matachana, modern, in perfect condition), which can hold 2-3 small boxes of instruments. They have another autoclave next to, which they use as a deposit for sterilised material.
The local team constantly washes and sterilises the material, in order to maintain a high rate of replacement. The sterile, disposable operating theatre linen, gowns, sheets and drapes, were brought by us.
OUR LIFE IN DANGBO
This week in Dangbo has been very intense. We have worked hard, and the whole group has been living together in a very healthy atmosphere. The alarm clock goes off at 7AM. At 7:30AM we are having breakfast in the hotel restaurant. Soluble coffee, tea with lemon, condensed milk, and a plate of omelette with vegetables and a roll of bread. The last few days, they even served us croissants and chocolate breads.
It is a pleasant 10-minute walk to the hospital and the day begins.
On Sunday morning we went to see the patients, and we organised the whole plan on two surgical tables, with about 5-6 patients with goitres on the general anaesthesia table, and about 8-10 patients with wall pathology on the spinal anaesthesia table, each day.
The only ‘down time’ we enjoyed was a walk around town on Sunday afternoon, and a quick visit to the beach on the Cotonou coast on Saturday afternoon, before embarking for home.
From Monday to Friday, our day basically consisted of operating from 8:30-14:30h and 15.30-22H. We stopped for an hour for lunch in the nuns’ dining room, and another hour at the end of the day for dinner. They served us a wonderful meal, salads for starters and a variety of dishes for main courses – they even made a Spanish omelette! And, of course, there was always cold beer, something that could be considered a basic necessity, considering the heat and the risk of dehydration associated with the intense work.
At the end of the day, we went for another night walk back to the hotel. Before falling asleep at around 23:30-24h, we only have time for a wonderful shower with buckets of cold water.
During the working day, it is quite hot inside the operating theatre. The only place where it is more comfortable is in the operating theatre, thanks to two air-conditioning units that run all day long.
All in all, our life in this campaign has been very pleasant, with a good atmosphere, a lot of work, and with the feeling that in Dangbo everything is ‘easy’. We leave with the feeling of having worked hard, of having participated in a great project, Hopital Albergue d’Amour Redemptour, led by Sister Opportune, and with the desire to return again. SAF will not miss its appointment, and I hope that we will be able to carry out more campaigns there next year.
3. CONCLUSION
3.1 Strengths of this site:
-Local organisation and staff. This is undoubtedly one of the best locations for SAF to work with.
-Recruitment.
-Quietness of the location.
-Short’ travel time from Spain.
3.2. Objectives for improvement:
-I believe that, with the acquisition of the new ventilator, a new room could be set up as an operating theatre for spinal anaesthesia, allowing 3 patients to be operated on at the same time.
-One or two stretchers in the room next to the operating theatre to make the transfer of patients and their stay there during post-anaesthesia recovery more comfortable. At present there is one transfer stretcher with wheels and one stretcher without wheels, with a broken backrest.
-New blood pressure cuffs on the monitors.
-Fix the air-conditioning unit in the operating theatre storeroom.
The Hernia International Mongolia 2024 mission was conducted over two weeks from 8 to 21 September.
The team consisted of members from Australia (Noha Ferrah, Cameron Dunlop, Richard Turner) and the UK (Steve Lindley, Bohdan Smajer). The first week was spent at Choir Hospital in Govisümber province situated in central-east Mongolia; the second at the Second State Central Hospital (a.k.a. National Diagnostic and Treatment Center) in capital Ulaanbaatar. Pre-mission liaison with the Mongolian surgeons was comprehensively handled by Dr Enkhee, who has vast experience in dealing with foreign teams and was always available to deal with any issues that arose.
The work experience
In Choir, our team conducted 17 consultations, leading to 14 operations on patients aged from 12 months to 72 years.
At the Second State General Hospital, we conducted 28 consultations and 19 operations on patients aged between 31 and 80 years. Patients at this hospital were admitted the day before proposed surgery, which enabled us to develop a team consensus on their management after we finished our day’s operating.
Days typically commenced with a ward round of previously operated patients. Aftercare was generally very good. We were impressed by the general stoicism of the patients, and the fact that all of those with incisional hernias came with their own fitted corsets.
Details of the operations performed are shown in the Table below. Incisional hernias predominated, with only 5 inguinal hernia repairs performed over the 2-week period.
Laparoscopy was available in both hospitals and local surgeons were keen to develop their skills in this; however, only a minority of cases were deemed suitable. Of note, 6 paediatric herniotomies were performed in Choir, due to a visiting Paediatric Anaesthetist.
Cases were generally cancelled if the team felt that the hernia was too complex for local capability, including the unavailability of optimisation techniques such as botulinum toxin. On departure, we were not aware of any significant postoperative complications.
At both hospitals, the program included dedicated teaching time, which included lectures with slides or videos, as well as an introductory session with the laparoscopic trainer. All operations performed were assisted by at least one local surgeon or trainee, who were keen to gain operative tips.
The visitor experience
Our Mongolian hosts, Drs Naraa and Sonor, Residents Tenuun and Miga, and many others, went to no end of trouble to provide us with a comprehensive cultural immersion, including:
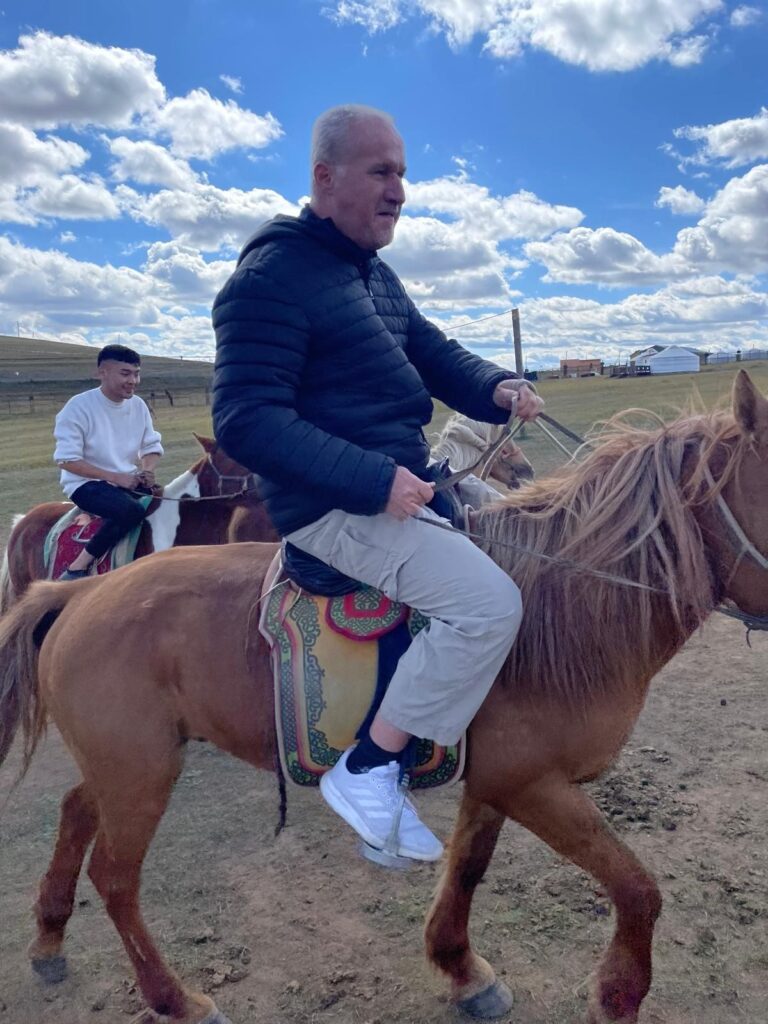
An afternoon spent in a ger on the road to Choir – sharing fermented horse milk and watching traditional sports.
An excursion to the Chinggis Khaan memorial outside Ulaanbaatar – with forays into camel/horse riding and archery
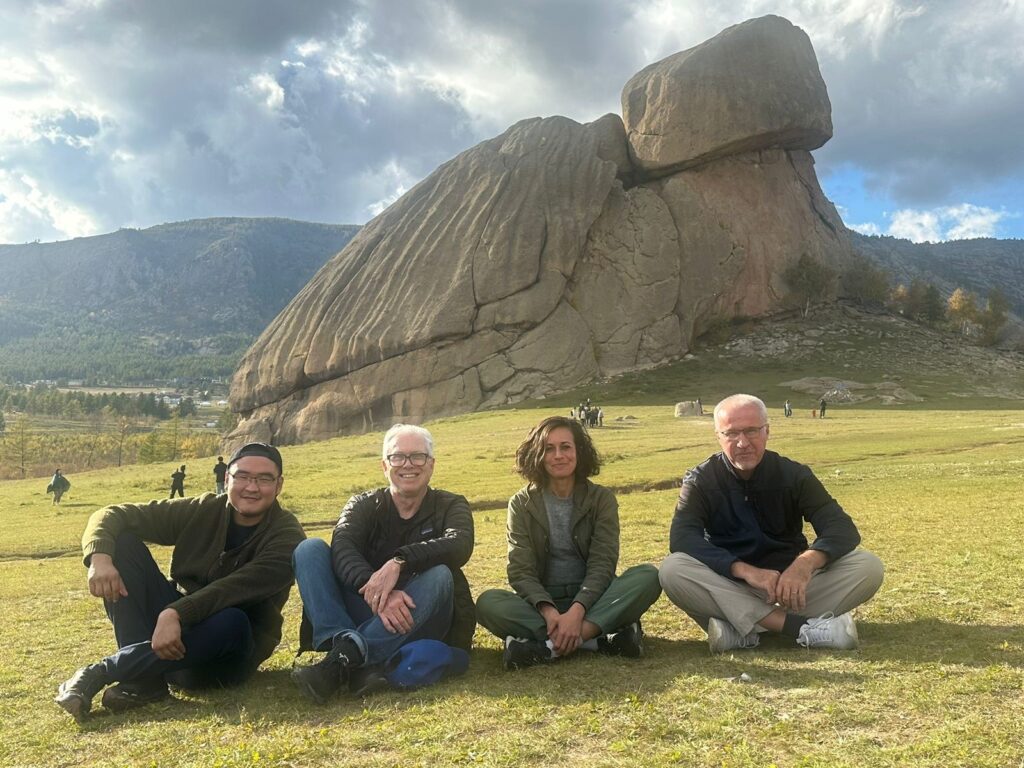
A visit to a Buddhist temple in the beautiful Terelj National Park
A variety performance with traditional music, singing, dancing, and eye-watering contortionism
A copious Mongolian Chinese banquet, hosted by Second State Central Hospital Director Dr Byambadorj – with vodka shots in the VIP room of a restaurant with possibly the largest self-revolving “lazy susan” in Asia.
We were most grateful for the transfers between Chinggis Khaan International Airport and our Ulaanbaatar hotel that were kindly provided by hospital staff. This must have been a considerable impost, given the permanently grid-locked nature of traffic in that city!
Advice for future teams
We were advised from the outset that the Mongolian health authority would not accept the low-cost sterilised mosquito net mesh usually provided by Hernia International – although in retrospect, this may not have been suitable for most of the hernias we were required to repair. Donations of commercial prosthetic mesh products must therefore be sought. Other key materials such as specific suture types and mesh fixation devices may also be lacking, especially in the rural hospitals. It is therefore advisable to bring supplies of these as well and liaise in advance with the Mongolian colleagues to ascertain precise requirements.
In our case, we owe thanks to Medtronic (prosthetic mesh), UPC Renewables (funding for purchase of laparoscopic trainer and sutures), the Royal Hobart Hospital (laparoscopic fixation devices), and the Bolton Hospital NHS Foundation Trust, UK (meshes and fixation device). The team leader should also confirm with the Mongolian side that Mongolian Customs has received documentation of what supplies are being brought into the country by HI team members – otherwise unwanted delays on arrival at the airport may occur.
Given the volume of incisional hernias presented to us, and that some were deemed out of scope for our mission, pre-assessment by the whole team is desirable. Ideally, this should be as early in the week as possible, so the whole week’s program can be planned and operations allocated according to expertise. It may even be possible to request advance e-referrals from local surgeons for complex cases, with CT images and clinical photographs.
As noted above, the Mongolian surgeons and resident doctors are keen for teaching both inside and outside the operating theatre, particularly for minimally invasive surgery and complex hernias. It is advisable to come prepared with a few PowerPoint lectures and videos, if possible. In theatre, be prepared to talk through the operations step by step, and supervise the assistant doing sub-tasks wherever possible.
In conclusion, the HI Mongolia 2024 mission was an excellent experience in collegiality and knowledge sharing. I daresay we would all be happy to do it again – and with each other!
Richard Turner
Team leader, Hernia International Mongolia 2024.
Table 1: Hernia operations undertaken at the Choir and Second State Central Hospitals, September 2024
Comprehensive Report on the Outreach by Liberia Physicians and Surgeons Without Borders (LPSWB) in Collaboration with Hernia International UK at C.B. Dunbar Government Hospital
Introduction
From June 25 to June 29, 2024, the Liberia Physicians and Surgeons Without Borders (LPSWB), in collaboration with Hernia International UK, conducted a free hernia surgery campaign at C.B. Dunbar Government Hospital in Banga City, Bong County, Liberia. This outreach aimed to provide essential surgical care to patients suffering from hernias, thereby improving their quality of life and reducing the burden of untreated hernias in the region. This mission marked the first collaboration between Hernia International and C.B. Dunbar Government Hospital.
Team Composition
The medical team comprised highly skilled professionals from various specialties:
Dr. M. Peter George – Consultant Surgeon, Team Lead
Dr. Ayun Cassell III – Consultant Urologist Surgeon
Dr. Abraham Ajami – Specialist Internal Medicine & Emergency Response
Dr. Michael Kempeh – Specialist General Surgeon
Dr. Arthur Wuoh – Specialist General Surgeon and Medical Director
Dr. Ambrous Fawenneh – Medical Officer
Dr. Brooks – Medical Officer in Rural Rotation
Momoh Sonnie – Nurse Anesthetist
Roger Corcor – Operating Theatre Technician
Mission Overview
Arrival and Preparation: The team arrived on June 24, 2024, and began preparations for the surgeries.
Surgical Campaign: Surgeries commenced on June 25, 2024, and continued until June 29, 2024.
Patient Recruitment: Dr. Arthur Wuoh, Medical Director and Specialist General Surgeon, was responsible for recruiting all patients who underwent operations.
Data Collection
Data collected during the mission was categorized to reflect various aspects of the outreach, including patient demographics, types of hernias operated on, surgical outcomes, and postoperative care.
1. Patient Demographics
Total Number of Patients Operated On: 108 procedures
Age Distribution of Patients:
Mean age: 31.69 years
Age range: 0.2 to 73 years
Age Group
Frequency
Percent
Cumulative Percent
0 – <10
23
21.3%
21.3%
10 – <20
15
13.9%
35.2%
20 – <30
14
13.0%
48.2%
30 – <40
16
14.8%
63.0%
40 – <50
16
14.8%
77.8%
50 – <60
9
8.3%
86.1%
60 – <70
10
9.3%
95.4%
70 – <75
5
4.6%
100.0%
Total
108
100%
100%
Gender Distribution of Patients:
Gender
Frequency
Percent
Cumulative Percent
Female
35
32.4%
32.4%
Male
73
67.6%
100.0%
Total
108
100%
100%
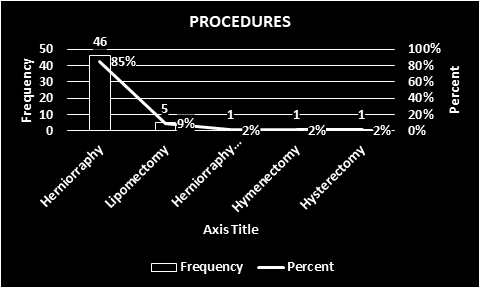
2. Types of Procedures
Procedure
Frequency
Percent
Herniorophy
51
47.2%
Herniotomy
11
10.2%
Lipomectomy
10
9.3%
Cesarian Section
9
8.3%
Hydrocelectomy
9
8.3%
Myomectomy
6
5.6%
Umbilica Hernia Repair
4
3.7%
Cystecyomy
3
2.8%
Hysterectomy
2
1.9%
Fistula
1
0.9%
Mayo Repair
1
0.9%
SUB-TAH
1
0.9%
3. Surgical Outcomes
Number of Successful Surgeries: 108 procedures
Complications Encountered: None
Length of Hospital Stay Post-Surgery: 1 night
Patient Satisfaction and Feedback: Very Good
4. Postoperative Care
Postoperative Recovery Protocols: Hernia International Standards
Follow-up Schedules: Managed by the Hospital Management
5. Anesthesia Given
Anesthesia Type
Frequency
Percent
Cumulative Percent
General Anesthesia (G/A)
36
33.3%
33.3%
Spinal Anesthesia (S/A)
72
66.7%
100.0%
Total
108
100%
100%
6. Diagnosis Percentages
Diagnosis
Frequency
Percent
Cumulative Percent
Adhesion
1
0.9%
0.9%
Bowel Aneste
1
0.9%
1.9%
BIH
5
4.6%
6.5%
Hydrocele
7
6.5%
13.0%
Infected Cyst
1
0.9%
13.9%
LIH
18
16.7%
30.6%
Lipoma
10
9.3%
39.8%
LISH
1
0.9%
40.7%
Myoma
9
8.3%
49.1%
Obstructed Labor
7
6.5%
55.6%
Ovarian Cyst
1
0.9%
56.5%
Previous C/S
1
0.9%
57.4%
RIH
36
33.3%
90.7%
RISH
2
1.9%
92.6%
Testicular Cysts
1
0.9%
93.5%
Umbilical
5
4.6%
98.2%
Umbilical Hernia
2
1.9%
100.0%
Total
108
100%
100%
7. Procedures Performed by Doctors
Doctor
Frequency
Percent
Cumulative Percent
Dr. Cyrus
2
1.9%
1.9%
Dr. Fawsenneh
16
14.8%
16.7%
Dr. George
35
32.4%
49.1%
Dr. Kempeh
35
32.4%
81.5%
Dr. Massaley
11
10.2%
91.7%
Dr. Wuoh
6
5.6%
97.2%
Dr. Yohn
3
2.8%
100.0%
Total
108
100%
100%
Summary of Findings
A detailed analysis of the data collected during the mission indicates a high success rate with minimal complications, reflecting the expertise and dedication of the medical team. Patient satisfaction levels were very high, and there were no significant complications encountered.
Conclusion
The collaboration between Liberia Physicians and Surgeons Without Borders and Hernia International UK at C.B. Dunbar Government Hospital was a significant milestone. This first mission successfully provided much-needed surgical care to numerous patients suffering from hernias, showcasing the importance of such outreach programs.
The team of collaborators began to be formed at the end of February 2024 under the leadership and coordination of Dra Teresa Butrón and under the umbrella of the Non Profit Organization “Cirujanos en Acción” (Surgeons in Action) and the collaboration of Hernia International Foundation. In a very short period of time, it could be formed a team of twelve people, including general and paediatric surgeons, paediatrics intensivist, anesthetists and nurses.
All volunteers collected all the consumable material needed for the campaign, including surgical gowns, drapes, surgical fields, sutures, meshes of different types and sizes, bladder catheters, sterile and operating gloves as well as drugs (local and general anaesthetics, muscle relaxants, antibiotics, opioids, analgesics, etc) and anaesthetic material such as spinal needles, epidural catheters, Laryngeal masks, endotracheal tubes and rest of the material.
The 12 de Octubre University Hospital, in Madrid, donated a large amount of medication including anaesthetics, analgesics, antibiotics and vasoactive drugs through the anesthesiologist of that hospital, Dr. Ana Hermira.
The University Hospital Virgen de las Nieves in Granada, through Silvia Montalbán, a nurse at the hospital, donated a large amount of material, including surgical gowns and sheets, electric scalpels and intravenous access equipment.
The air tickets were taken through Angelis (freelance of Halcon Viajes Company) with the company Turkish Airlines, which allowed the transport of 2 bags of 23 kg per person + cabin baggage.
VISA. Without a doubt, obtaining VISA from Nigeria’s Embassy in Madrid, was the greatest difficulty that we had to face and that seriously jeopardized the completion of the campaign. Thanks to the efforts of Teresa Butrón and Dolores Delgado and their persistence we were able, just three days before leaving, to obtain VISA for Nigeria for all the members of the team. It is possible to apply for the VISA online and make the payment and after that it is necessary to go the Nigeria’s Embassy in Madrid to present the VISA application form, the invoice and the passport. Therefore, all the cooperators living outside of Madrid had to send their original passports by mail to one of the team members in Madrid to present them all together as a group. We got the VISAS only three days before leaving for Nigeria. For all of those reasons it seems advisable and it is our recommendation, to start the process at least six weeks in advance.
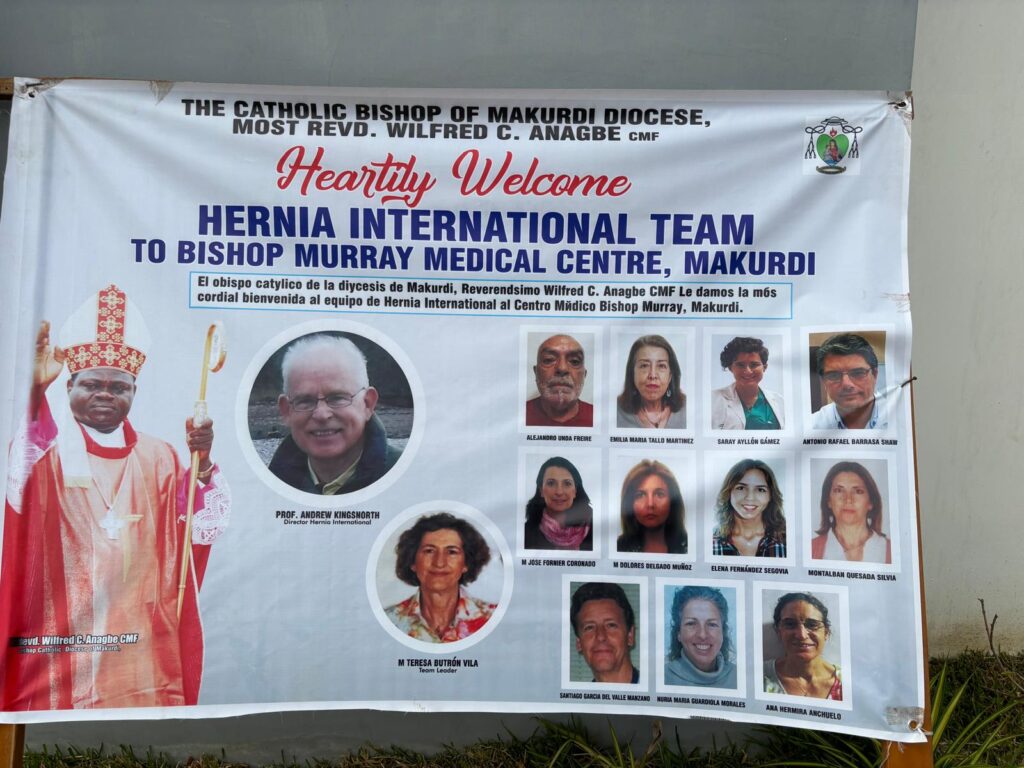
Dr Austin Ella, Associate Director Program Management from Catholic Caritas Foundation of Nigeria (CCFN) and Catholic Secretariat of Nigeria Building was our local contact in Nigeria and our interlocutor with Bishop Wilfred Chikpa Anagbe.
The group of volunteers left Spain from different cities (Málaga, Valencia, Madrid) between Friday and Saturday, April 19 and 20, 2024. Ten of the team members met at the Istanbul airport while two of our surgeons arrived at Abuja a day before the rest of the team
The campaign ended on Saturday, April 27, 2024 and we arrived to Spain on Monday 29th.
PATIENTS.Altogether 155 patients were operated on during the campaign period
ADULTS PATIENTS: A total of 93 surgical procedures were performed in 80 adult patients. There were 14 females and 66 males. Age ranged from 16 to 76 years (median 50; interquartile range 36-62). The following procedures were done:
Lichtenstein: 69 cases
Nyhus: 10 cases
Lipoma removal: 3 cases
Pre-peritoneal mesh repair: 2 cases
Rives-Stoppa: 2 cases
Hydrocelectomy: 2 cases
Reinforced suture + umbilical prefascial hernia repair + fascia plication: 1 case
Nuck’s cyst removal: 1 case
Onlay: 1 case
Orchiectomy: 1 case
Haemorrhoidectomy: 1 case
Most of the cases under spinal anesthesia (77 patients), saddle block (1 patient) and local anaesthesia plus sedation (2 cases)
PAEDIATRICS PATIENTS. 99 procedures were performed in 75 paediatric patients. Seventeen females and 58 males. Age ranged from 3 months to 16 years (median 6; interquartile range 3-10).
Herniorrhaphy: 92 cases
Herniorrhaphy plus hydrocele: 1 case
Hydrocele: 4
Orchidopexy: 1 case
Dermoid cyst resection: 1 case
Several cases of the initially scheduled were left without being operated on due to the lack of enough time.
All the members of the team agreed about the need to know more in depth the scheduled cases to made a more appropriate surgical list of patients. It was the first mission there in Makurdi and probably the situation will improve in future missions.
We also had the opportunity to participate in two cases of urgent caesarean section: fetal distress in one case and previous caesarean section in the other. Both patients were operated under spinal anaesthesia and two general surgeons from CeA helped Dr Thadeus Aende in the surgery and also did it the nurses of the team. It was very gratifying for all of to participate in that task and see the good evolution of mothers and newborns.
COMPLICATIONS: Once the team left Makurdi Hospital, the follow up of patients was done by Dr Thadeus Aende, a local doctor. Up to now, there have been four early minor complications: one adult patient experienced a recurrence of his inguinal hernia and, in the paediatric population, a boy developed a wound abscess drained while the team was still in Makurdi, one more a reactive hydrocele and, lastly, a possible recurrence of a hernia or simply a local edema difficult to know from the pictures Dr Thadeus Aende sent to the paediatric surgeons.
Nigeria’s economy is the second-largest in Africa, the 39th-largest in the world by nominal GDP, and 27th-largest by PPP. However, the GDP per capita places it in 149th place out of 196 countries and the Human Development Index prepared by UN which shows the standard of living indicates that Nigerians are among those with the worst quality of life in the world.
Benue state was created on February 3, 1976. It lies roughly in the middle of the country. Benue has a population of more than 4,5 millions inhabitants. The state comprises of several ethnic groups being The Tiv the dominant ethnic group, occupying 14 local government areas, while the Idoma and Igede occupy the remaining nine local government areas. Most of the people are farmers while the inhabitants of the riverine areas engage in fishing as their primary or important secondary occupation. The people of the state are famous for their cheerful and hospitable disposition as well as rich cultural heritage. Makurdi, the State capital was established in the early twenties. Being a river port, it attracted the establishment of trading depots by companies such as UAC and John Holt Limited. Its commercial status was further enhanced when the Railway Bridge was completed and opened in 1932. In 1976, the town became the capital of Benue State and presently serves also as the headquarters of Makurdi Local Government Area.
THE TEAM was composed by a total number of 12 volunteers:
General Surgeons: Teresa Butrón Vila (team leader). Antonio Rafael Barrasa. Saray Ayllón Gámez. Elena Fernández Segovia.
Paediatric surgeons. Alejandro Unda Freire. Mª Dolores Delgado Muñoz.
Paediatric intensivist. Emilia María Tallo Martínez.
Anaesthesiologists. Ana Hermira Anchuelo. Santiago García del Valle
Nurses. Mª Josefa Fornier Coronado. Nuria Guardiola Morales. Silvia Montalbán.
LOCAL STAFF. El Dr Thadeus Aende was the only doctor available at the hospital even though there were a large number of volunteers carrying out tasks of organization and identification of the population. Father Peter Paleva was the Area Health Coordinator. Mr Nicholai Ahor was the Administration Secretary.
HOSPITAL. It is a small building all in a single height, with several wards for adults, men and women, and children. It has a laboratory for basic determinations and a microbiology laboratory with basic capacity to perform cultures and diagnostic test for pathologies such as malaria and HIV. The room we use as an operating room is a large elongated space, equipped with air conditioning (the only space in the hospital except offices), without running water and equipped with minimal material: oxygen cylinders, two basic monitors (ECG did not work correctly) and 3 very rudimentary operating tables, one of then without the possibility of modifying height or changing the position of the patients. There was no anaesthesia machine available. There was no recovery room so the adult patients had to go directly to the ward, not far from the OR. For the children Dr Emilia Tallo created a small room as a space where to look for the children several minutes after the operation. The heat and humidity in that space was terrible and that made Emilia’s work very difficult and to be grateful for all of us. Several portable pulse oxymeters led by cooperators alleviated partially the monitoring deficit.
EQUIPMENT.Surgical instruments available at the Bishop Murray Hospital such as forceps, separators or scissors are not in very good condition and no suitable sizes for some of the longer and more aggressive interventions. It was completed with the paediatric surgical material carried by Alejandro Unda. There were
2 diathermy generators, one from the own hospital and one brought from Abuja and the team could transport 2 more units from Spain even though we have to use only one of them. The surgical lights were scarce and very poor in intensity and difficult or impossible to handle.
ANAESTHESIA. The lack of an anaesthesia machine made the task of Dr Ana Hermira and Dr Santiago Gª del Valle very difficult since they had to combine spinal anaesthesia with regional anaesthesia of the trunk with sedation or even general anaesthesia under spontaneous breathing. We made Dr Ella aware of the need to acquire a simple anaesthesia machine for the future campaigns and, thus, a report was sent to him with a description of the minimum characteristics and capabilities that anaesthesia should have.
ASEPSIS:Sterilisation was carried out with a heat-operated autoclave in a room adjacent to the operating room.
OUR DAILY LIFE
We arrived at Abuja International Airport on Saturday 20 April at 20:00. There were no difficulties with customs formalities and from there we were transferred to the Catholic Residence from Bishop Office and Caritas Organization only a few kilometres away from the airport where we met the rest of our colleagues. In that residence we had dinner and spent the first night.
Early in the morning of Sunday 21th April we went to Makurdi by car and it took 4 four and a half hours to made the 280 kilometres. Once at the hospital we had a colorful and pleasant welcome ceremony after which they offered us a meal to, immediately afterwards, inspect the operating rooms and the rest of the hospital, review the available material and unpack and organize the large amount of material that we moved from Spain.
We had lunch in the hospital and the food was of good quality but it is important to warn the cooker, Rosario Joyn Egbol and Dr Celeste Conde (also Medical Director of the Hospital), not to add spice. Delicious were also the great variety of mangoes we could taste.
After the daily work we took dinner at the residence. The rooms were comfortable with shower and, most importantly, air conditioning. It is important to take with you some towels.
We worked during 6 days (Monday to Saturday inclusive) from 8:00 to 20:00 or even later several days. On Wednesday 24th the Bishop offered us a nice dinner in the garden of the residence. We had no time even to visit the city center neither the riverside of the imponent Benue River.
On Sunday 28th we were invited to a religious ceremony and after that we came back to Abuja’s airport. The trip was made difficult by two car breakdowns that delayed our arrival at the airport to such extent that we almost missed our flight and were allowed to carry only our hand luggage and had to leave the rest of the equipment in Abuja under the care of Dr Austin Ellla who was later in charge of sending all the material back to Spain several days later.
CONCLUSION
Strengths of this place: Probably there is a huge amount of population who would benefit of a surgery from CeA. The people were very warm towards us and expressed continuously their gratitude. A lot of local volunteers, poor organized ass it was the first mission but they helped us a lot with the management of patients and families.
Improvement objectives: It would be very useful for future campaigns to have an anaesthesia machine and a new basic monitor of vital signs. It is desirable to improve the surgical lights as well as the surgical tables because they must have the capacity to vary their height and change the position of the patients during surgery. Also is important to improve the cars for the transport from Abuja to Makurdi and back to the airport since the space for the people and equipment was very limited. Have running water in the operating room, as occurs in other areas of the hospital, could facilitate work and help reduce the chance of surgical infections.
BUDGET:
COST FOR PERSON:Flight tickets between 600 and 750€. Hotel and maintenance provided by the local organization without cost. VISA 100€. Total amount around 700-850€ per volunteer.
We started the trip on the morning of 27/04. 7 members of the group will leave from Vigo and 1 from Gran Canaria. We have a long journey to our final destination, the Police Hospital in Freetown, Sierra Leone. We meet in Madrid, where David and Nuria are waiting for us to deliver the diathermy generator that we have to take with us. In the end we check in 11 bags of between 20 and 23Kg of material. We fly with Royal Air Maroc, with a stopover in Casablanca.
We bought the plane tickets through Angelis, an agent of Halcon viajes.
To enter the country you need a Visa, which can be easily obtained online via the link on the Spanish foreign ministry’s website. It costs $85 and takes a few days to be issued
1.2 ADULT PATIENTS:
As a ventilator was not yet available, only pathologies that were amenable to spinal anaesthesia and local anaesthesia and sedation were performed.
Surgery was mainly performed on abdominal wall pathology, hydroceles and large lipomas.
1.3 PAEDIATRIC PATIENTS:
No paediatric patients were operated on in this campaign, as general anaesthesia cannot be performed.
Inguinal hernia: 91, all repaired with Lichtenstein technique
Epigastric hernia: 8
Umbilical Hernia 3
Femoral Hernia 2
Hydrocele: 20
Testicular tumour: 2
Lipomas: 19
Mandibular tumour: 2
Sebaceus cyst: 1
Oral mucosal lesion: 1
Urgent reviews: 3
1.5 Total patients
1.6 COMPLICATIONS:
As complications, 3 patients required immediate postoperative reoperation: 2 haematomas in giant inguinoscrotal hernias and 1 seroma of 1 giant sebaceous cyst on the scalp. All complications resolved without further incident. To date, one month after our return, we have not been informed of any incident.
2. CAMPAIGN REPORT
2.1. THE PLACE
The hospital has 2 operating theatres, including a sterilisation room. The surgical material available is sufficient for hernias and other simple pathologies, but there is no material for laparotomy, thyroid surgery or surgery on children.
There is air conditioning in the operating theatres, which is to be welcomed, although due to the constant power cuts, it does not cool as much as we would like.
They have an autoclave for sterilisation, which they hardly use, because they find it too slow. They use pressure cookers, which worked correctly, except for one day, when we were stopped for 3 hours due to a problem with the closure of the cooker, which was finally solved.
It has 2 diathermy generators that work correctly, but only one of them can be used, because the other one does not have a grounding plate (it is an old, metallic plate). We used the generator we took with us and the other one, which worked properly for 4 days. Then the connection to the plate broke and they couldn’t fix it, so we spent 1.5 days with only one scalpel.
They have 3 mixed rooms, where patients are accommodated before and after the operation. There is a permanent nursing staff there, although the care is quite poor, given the poor training of the local staff and the limited means available.
2.1. THE TEAM
General surgeons:
Ana María Gay Fernández
Enrique Moncada Iribarren
Cristina Roque Castellanos
Paula Fernández Rodríguez
Anesthesiologist:
Miguel Ángel Pereira Loureiro
Yolanda Sanduende Otero
Nurses:
Verónica González Casal
Eva Sánchez Hernández
2.2. THE LOCAL STAFF
Dr Konteh, the hospital director, who is in charge of organising the campaign.
A surgical assistant (Kelly), who can help in the surgeries.
A preventivist, who is very helpful, and who helps us a lot in the operating theatre, especially in speeding up sterilisation and getting supplies when we run out.
The male nurse Francis, a hard worker, is also a great help in everything.
The nurses in the rooms are in charge of taking IVs from the patients before the operating theatre and post-operative care.
2.4 EQUIPMENT
Diathermy generators: 2. Neither of them have a plate and ours cannot be attached.
Operating theatre lamps: they have 2 lamps, which are quite deficient. One of them stopped working on the 3rd day of the campaign, and it was not possible to fix it. It is essential to carry a headlamp for the surgeries.
Consumables: sterile surgical gowns and drapes are not available. They have equipment to take peripheral lines and IV systems.
Medication: poor availability, although some things we ran out of they did get, such as antibiotics.
2.3. ANAESTHESIA
In the surgical block we had only 1 monitor that allowed us to measure O2 saturation and PANI, but it did not have electrocardiographic recording.
For this reason, we brought an automatic blood pressure monitor and a portable pulse oximeter that allowed us to have minimal monitoring on the second operating table, material that we left at the hospital in Freetown.
This double monitoring allowed us to tansfer 2 patients simultaneously to the 2 surgical tables that we placed in the same operating theatre, where we proceeded to perform spinal anaesthesia and some deep sedation, in cases of supra-umbilical pathology (some lipomas).
There were 2 oxygen concentrators that worked properly and an oxygen bullet to which we connected the ambu, but which we did not have to use at any time.
In the operating theatre there was also 1 very old aspirator.
Outside the operating theatre they had a NON-functioning Aestiva Datex-Ohmeda ventilator, so no other anaesthetic option other than local or regional, or light sedation, was ever considered. Stored in a corridor, there was another older ventilator which was also non-functional.
On arrival, the equipment available was generally scarce: some O2 goggles and ventimask, and little else.
The campaign brought from Spain all the material and medication necessary to perform intradural anaesthesia/local infiltration (lidocaine, bupi isobara and hyperbara, mepivacaine, prilocaine), sedation (propofol, ketamine, fentanyl, midazolam), as well as iv/vo antibiotics, and general emergency medication (atropines, adrenalines, amiodarone, antihistamines, corticoids in different doses, antiemetics). As for analgesics, in addition to opiates, we carried conventional IV analgesia for each operation, and oral analgesia for the first 24 hours postoperatively.
There was no stock of medicines.
As we had calculated the campaign for about 100 patients, and we exceeded expectations, we ran out of spinal needles, antibiotic prophylaxis and benzodiazepines, material and medication provided by the hospital itself, although the prophylaxis had to be done with ceftriaxone, and the needles were 24G-25G thick gauge without an introducer, which posed us greater technical difficulty on occasion.
The activity we carried out was:
Type Anaesthesia
Type of surgery
A. Spinal
Intradurals
110
Hernias and infraumbilical abdominal wall
Sedation
Local + Sedation
16
Lipomas, epigastric hernias
Deep Sedation
4
large and/or deep supra-umbilical or dorsal lipomas
Total
130
Tras la intervención incluíamos analgésicos (2 AINES y opiaceo o asociacion de rescate) para las primeras 24 h del posoperatorio.
No tuvimos complicaciones importantes y entre las leves, escasa o nula hipotensión con algún episodio de náuseas/vómitos, y algún caso de analgesia insuficiente.
2.6. ASEPSIS AND SURGICAL SUPPLIES
Sterilisation: autoclave. Pressure cookers
Surgical instruments: there is material for small operations, such as hernias. There are few separators. There is no Roux type. There is also no specific material for thyroid or child surgery, so if at any time this type of surgery is considered, it will be necessary to bring material.
2.7. OUR LIFE IN FREETOWN
We land at Freetown airport at 2:00 a.m. Dr Konteh, director of the hopistal and organiser of the campaign, is waiting for us there with Abu, a security policeman who accompanies us to the hospital every day. We collect our luggage and pass through customs without incident thanks to Dr Konteh’s help. Then we go to catch the bus (about 15 minutes), which takes us to the ferry, which takes about 45 minutes. We arrive at the hotel at about 5am. After a few hours rest we head to the hospital. While the nursing and anaesthesia team open the material packs and get everything ready for the surgeries, the surgical team is ready to see the potential surgical patients. Patient recruitment was extensive. On arrival we had more than 300 surgical candidates. However, no one had done a screening, so we saw many non-surgical pathologies, or pathologies that could not be operated on in a campaign where general anaesthesia is not possible. Finally, after many hours of seeing patients and after recruiting 145 patients for surgery, we decided not to continue with the screening, so that we could start operating that same day, late in the afternoon, almost at night. We scheduled the surgeries for later days.
The day after our arrival we were received by the Chief Inspector of Police (Mr. William Fayia Sellu), in a brief ceremony held at the police headquarters, and he gave us our permits to work in the country.
Thus began a very hard campaign, with intense heat during the day and night, working daily from 8 in the morning, extending most days until more than 9 at night, since an average of 25 patients were operated on per day. In the end, despite having two operating theatres, we decided to use only one, with two tables, to speed up the work.
We started the day with breakfast at the hotel. They provide coffee, powdered milk, juice and you can order omelettes and pancakes. At 8 a.m. we are picked up by Dr Konteh with Abu, a 15-minute drive to the hospital.
On arrival, while the first patients are being anaesthetised and everything is getting underway, the surgeons visit the patients from the previous day, so that they can be discharged and make room for the patients who will be operated on that day.
We make a short stop for lunch. Pizza, chicken, pasta and a few other things can be ordered from a nearby restaurant. The local staff bring them every day, although you have to order well in advance, so on many days we just ordered bread and fruit and added cold meats that we had brought in our suitcases.
In the evening we dine at the hotel, having ordered our orders in the morning before we left. The offer is similar to that of the lunch restaurant: rice, pizza, chicken or pasta.
On the 4th day of the camp, the connection of the scalpel plate they have in the hospital broke, and it was not possible to fix it, so we were left with only one scalpel. We decided to continue on 2 tables, exchanging the scalpel that we had brought with us, as one surgery was finished, we started on the next table, with everything already prepared. This, of course, delayed us a lot, and it was impossible for us to keep to the schedule, which was already complicated to carry out. Therefore, we prioritised patients with hernias and suspended several lipomas that do not pose any risk and can be operated on in successive campaigns.
Finally on the last day they got another generator that worked properly and we operated on the remaining 11 patients, somewhat simpler hernias than in the previous days, to avoid complications. After finishing all the work, we collected and packed the diathermy generator and some more material to take back to Spain.
After resting for a while at the hotel (they let us stay in the rooms until the afternoon), Dr. Konteh and Abu picked us up to take us to the beach area, where they had prepared a farewell dinner for us. Beforehand, we met up at the hotel with my colleague and friend, Dr Marta Lado, an internist working in Sierra Leone, with whom it was impossible to meet for the rest of our stay, as our working days were too long. I met Dr Lado almost 20 years ago when we were both training in Spain. Her eagerness to train in infectious diseases took her to Sierra Leone 10 years ago. She came for a few months, but stayed during the Ebola outbreak at the time, and the country and its people got to her. She works with an American NGO (Partners in Health), carrying out health plans, as well as participating in the WHO’s outbreak emergencies group. By coincidence, Dr Lado was Dr Konteh’s mentor, so she is also joining us for the farewell dinner. It is a great pleasure and honour to have her and her knowledge of medicine and the country we are in. She can certainly be a support in future missions if needed.
During dinner, we are given gifts: a police T-shirt and a notebook with our name engraved on it. After dinner they play music and we dance until it is time to leave for the airport.
Dr Konteh accompanies us there, and thanks to his contacts, we avoid paying the departure tax, which is about 100 euros per person.
The return journey is uneventful until we arrive in Madrid, where we realise that one of the checked-in bags has not arrived. We recover it in Vigo that same week.
And now back, with the satisfaction of a job well done, we bid farewell until the next one. This mission has been particularly hard at times, with many hours of work, more than expected, with a lack of means and material, as well as a lot of heat. But as always happens in this type of campaign, the team spirit and mutual support, makes us draw strength from nowhere, to continue and that everything runs smoothly. Thanks to all the team, for the effort and the desire, and above all for coming back for another year…
CONCLUSION
3.1 Strengths of this place:
Sierra Leone is a country with a very poor health system. There are few doctors, and especially few surgeons and almost no anaesthetists. As a result, there is a huge number of patients, adults and children, who are potentially surgical. The Police Hospital, despite its shortcomings, is prepared for such campaigns. Dr Konteh is able to organise the campaigns and solve problems as they arise. The hospital staff is well adapted to the work, improving as the campaign progresses.
3.2. Improvement objectives:
– Prior screening of patients is essential. To rule out non-surgical pathologies and inoperable surgical pathologies during the campaign. It is very difficult to see such a large number of patients in such a short time, and above all, it is a significant waste of time, as more than half of the patients we screened in this campaign had no surgical pathology, or were not susceptible to surgery during the campaign due to the type of pathology.
– Improve pre- and post-operative care: in future campaigns it would be interesting to have nursing staff who can instruct local staff in this care: post-operative analgesia, wound care, correct channelling of IVs, taking of vital signs, etc., especially if the aim is to operate on more complex pathologies, as the knowledge of local nursing staff is very limited.
– Obtain a respirator that works properly.
– In future campaigns, if a respirator and a monitor can be obtained, three simultaneous operating tables could be set up.
4. BUDGET:
4.1. COST PER PARTICIPANT:
Participants travelling from Vigo, single room hotel: 2.021,10
Participants from Vigo, double room: 1.839,25
Participant from Gran Canaria, single room: 2.009,26